Download
1 / 37
580 likes | 1.6k Views
Vesiculo-Bullous Disorders. Definitions. Vesiculo-Bullous Disorders : group of skin diseases in which blistering in the form of vesicle or bullae occurs as a primary event either by genetic mutation or autoimmune response Vesicle: visible accumulation of fluid which is <0.5cm in size

E N D
Definitions Vesiculo-Bullous Disorders : group of skin diseases in which blistering in the form of vesicle or bullae occurs as a primary event either by genetic mutation or autoimmune response Vesicle: visible accumulation of fluid which is <0.5cm in size Bulla: visible accumulation of fluid which is >0.5cm in size
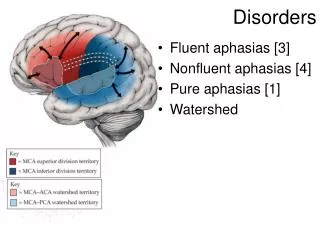
Classification A: Depending upon the site of blistering
Classification A: Depending upon the site of blistering
Classification B: depending upon cause • Autoimmune: Pemphigus, Pemphigoid, Dermatitis herpetiformis, Pemphigoidgestationis, Bullous SLE, Linear IgAdermatosis, Epidermolysisbullosaacquisita, Paraneoplasticpemphigus, Chronic blistering disease of childhood • Familial: Hailey Hailey disease, epidermolysisbullosa • Infectious: Varicella , herpes zoster, herpes simplex, candidiasis, bullous impetigo, bullous scabies. • Others: Burns, diabetic blister, TEN, SJS, Fixed drug eruption, Porphyrias, Bullouserythemamultiforme
Pemphigus • “Pemphix” in Greek means ‘Bubble’ • Chronic autoimmune bullousdermatosis • Immunopathologicallycharacterised by auto antibodies directed against the cell surface of epithelial cells
Pemphigus Epidemiology • 4th - 5th decade, M=F Etiology • Genetics: HLA DRB1, HLA DQB1 • Antigens: Desmogleins, desmocollins and desmoplakins present in the desmosomes act as the auto antigens • Antigen: Desmoglien1, Desmoglien3
Pathogenesis Circulating autoantibodies bind to cell surface lysis of intercellular cement substance acantholysis intraepidermal blister The blister cavity consists of mainly acantholytic cells
Clinical features • Thin walled flaccid bullae that rupture easily to form painful raw surfaces with tendency to spread; long time to heal • Sites: Starts in the oral cavity; then the groins, genitals, axillae, scalp, face, neck • Nikolsky’s sign: Positive, shearing stress applied to bony prominences on normal skin away from the lesion causes separation of the epidermis from the dermis • Bulla spread sign: Vertical pressure causes extension of blistering into the surrounding apparently normal skin
Diagnosis Tzanck smear • Acantholytic cell - Large round cell with hyperchromatic nucleus and perinuclear halo due to peripheral condensation of cytoplasm Histopathology • Supra basal cleft with acantholytic cells • Tomb stone appearance • Perivascular infiltrate of lymphocytes, neutrophils Immunofluorescence • Intercellular IgG and C3 deposits showing (Fishnet or Honey-comb pattern)
Treatment Systemic: • Steroids (mainstay of treatment) 1.5-2 mg/kg/day • Anti metabolites : Azathioprine, Cyclophosphamide, Cyclosporine • Pulse therapy: Dexamethasone - Cyclophosphamide pulse (DCP), Methyl-prednisolone pulse • Others : Plasmapheresis, Iv GammaglobulinsDapsone, Nicotinamide and Tetracycline, Antimalarials
Course and prognosis • Lesions subside with hyperpigmentation; with few recurrences and requires a longterm maintenance therapy • The most common cause of death: Septicemia and pulmonary embolism
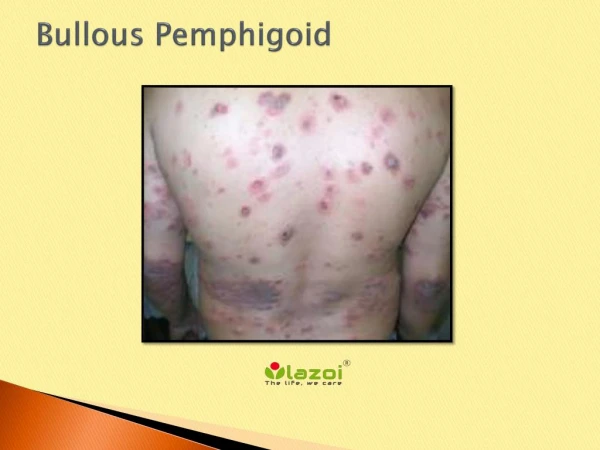
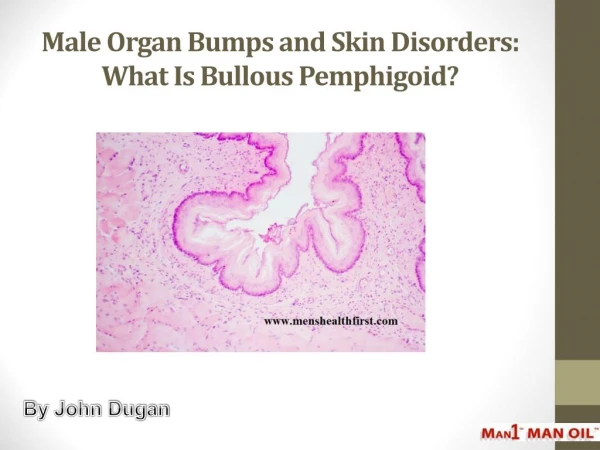
Bullouspemphigoid BullousPemphigoid is an • acquired autoimmune blistering disease of the elderly • characterized clinically by tense bullae • histopathologically by sub-epidermal bullae • immunopathologically by deposition of antibodies and complement along the basement membrane zone The term bullouspemphigoid was termed by Lever in 1953
Etiology Epidemiology • Age-60 to 75, M=F Etiology • Genetics: HLA DQ7, HLA DRB1 • Antigens: BPAg1(230 kDa) and BPAg 2(180 kDa) present in hemidesmosomes act as autoantigens • Antibodies: IgG, IgA, IgE
Pathogenesis Circulating antibodies bind to the lamina lucida activate the complement pathway eosinophils accumulate in dermis adhere to basement membrane zone (BMZ), release destructive enzymes BMZ separates Sub-epidermal blister is formed
Clinical features • Large tense sub-epidermal bullae on normal or erythematous base → on rupture form large denuded areas with tendency to heal • Urticarial plaques and patches with tendency to central clearing • Nikolsky’s sign: negative • Modified bulla spread sign: positive • Sites : Lower abdomen, inner thighs, groins, flexural aspect of limbs. Mucosal surfaces are involved in 10- 40% cases • Association : Malignancy, diabetes, ulcerative colitis, multiple sclerosis
Diagnosis • Tzanck smear : Plenty of eosinophils • Histopathology : Epidermis is usually normal Sub epidermal bulla filled with fibrin and eosinophils Dermis shows infiltrate of eosinophils, mononuclear cells and neutrophils • Immunopathology : C3, IgG, IgA, IgM seen along BMZ and in circulation
Treatment • Topical : Steroids • Systemic: Steroids 40-80 mg/day and tapered when disease under control Dapsone Tetracycline and Nicotinamide Immunosuppressants • Others: Plasmapheresis IV Gamma globulins
Prognosis • Benign self limiting disease lasting from months to years • Mortality rate less after advent of steroids • Most common cause of death is usually some underlying associated disease
Dermatitis Herpetiformis (DH) A rare chronic blistering disease of the skin characterized by: • Intensely pruritic grouped vesicles on an erythematous base • Granular IgA deposits on the dermal papillae on direct immunofluorescence • Association with gluten-sensitive enteropathy DH was first described by Duhring in 1884
Etiology Epidemiology • Age-20 to 40 yrs , M=F, Whites > Blacks/Asians Etiology • Genetics: HLA B8, DRw17 and DQw2 • External factors: Gluten containing diet like wheat, barley, oats and rye • Antigen: Gut epithelial antigen that cross reacts with skin • Antibodies: IgA directed against gliadin and autoantigens like reticulin and endomysium C3, IgG, IgM may be seen
Pathogenesis Gluten or its fragments are taken up by antigen presenting cells like lymphocytes activation of cytokines and inflammatory cells plasma cells release IgA2 directed against gliadin cross-reacts with autoantigens of skin and gut like reticulin, endomyosium
Clinical features • Severely pruritic grouped, papulovesicles on erythematous base • Sites: Symmetrical involvement of extensor aspect of knees, forearms, axillae, shoulders, sacrum, buttocks, face, nuchal area and on scalp • Associations: Gluten sensitive enteropathy, autoimmune diseases like diabetes, thyroid disease, pernicious anemia
Diagnosis • Tzanck smear: plenty of neutrophils • Histopathology: Neutrophilicmicroabscesses in dermal papilla with sub-epidermal vesicle • Immunopathology: Clinically normal skin on forearm or buttock shows granular IgA deposits in the dermal papilla. IgM, IgG may also be found
Treatment • Strict gluten free diet • Systemic steroids not the mainstay of therapy • Dapsone 100-200 mg/day • Sulphapyridine 1.5 g/ day • Tetracycline with nicotinamide • Colchicine when the above drugs are contraindicated
Prognosis • Disease present life long; with remissions and exacerbations • Strict gluten free diet causes remission of the skin and gut disease • About 10%-15% have spontaneous remissions • Increased risk of developing gastro-intestinal tract lymphoma
Epidermolysisbullosaacquisita (EBA) EBA is a mechanobullous disease of the elderly characterized by • Sub epidermal blistering on histopathology • Tissue bound and circulating anti bodies to type VII collagen Etiology • Genetics- HLA DR2 • Antigen- 290 kDa protein in type VII collagen (found in basement membrane zone) • Antibodies - IgG
Pathology The antigen antibody complex cause • direct destruction of anchoring filaments (non-inflammatory type) or • inflammatory response via complement system activation (inflammatory type) This causes the BMZ split and thus a sub epidermal blister
Clinical features 4th to 6th decade, M=F Non-Inflamatory type • Flaccid blisters over the trauma prone areas • Heal with scarring, milia and hyperpigmentation • Cicatricial alopecia and dystrophic nails seen Inflammatory type • Tense blisters and urticarial plaques on erythematous base that heal without scarring • Sites: Dorsa of hands and feet, elbows, knees • Associations: SLE, inflammatory bowel disease
Diagnosis • Histopathology • Sub-epidermal blister with or without lymphocytic infiltrate • Immunopathology Linear deposition of IgG, C3 and sometimes IgM, IgA Salt - splitting technique : Antibodies on dermal side
Treatment • Steroids in combination with dapsone/ sulphonamides (first line) • Colchicine • Cyclosporine • IV immunoglobulin
Prognosis • Chronic protracted disease with remission and exacerbations • Inflammatory type is amenable to treatment • Non-inflammatory type is difficult to suppress • Rarely the disease may remit spontaneously
Approach to vesiculobullous disorders • Clinical history and classical features • Tzanck smear • Histopathology : to find out the level of blister and type of cellular inflammatory infiltrate • Immunofluorescence : both direct and indirect methods for autoimmune bullousdermatoses