Download
1 / 20
200 likes | 211 Views
Explore how Magnetic Iron Detector (MID) offers non-invasive whole liver iron measurements for thalassemia and hemochromatosis patients, aiding in therapy management. MID provides reliable results comparable to existing techniques but is more affordable and user-friendly. The MID instrument, operating at room temperature, shows promising results in diagnosing liver iron overload and monitoring chelation therapy, simplifying clinical practices.

E N D
THALAS Biomag 2006 - 15th International Conference on Biomagnetism August 20 - 26, 2006 Vancouver, BC, Canada MAGNETIC IRON DETECTOR (MID) WHOLE LIVER IRON OVERLOAD MEASUREMENT BY A NON CRYOGENIC MAGNETIC SUSCEPTOMETER Mauro Marinelli1,2, Piergiorgio Beruto1, Barbara Gianesin1,2, Antonella Lavagetto3, Martina Lamagna3, Eraldo Oliveri2, Maria Luigia Saccone1, Giuliano Sobrero2, Laura Terenzani3, Gian Luca Forni3 1Physics Dept. University of Genova, Italy, 2National Institute of Nuclear Physics (INFN) Genova,3Centro della Microcitemia e Anemie Congenite, Ospedali Galliera, Genova, Italy
Abstract Assessment of body-iron accumulation is essential for managing therapy of iron-overload in diseases such as thalassemia, hereditary hemochromatosis and other forms of severe anemias. At present, the gold standard to determine liver-iron concentration (LIC) is the invasive liver needle biopsy; it might lead to large error, in assessing iron burden, due to the heterogeneous distribution of iron deposition in the liver. SQUID bio-susceptometer and MRI are currently the only non-invasive validated methods for LIC measurements. The susceptometer presented herein measures directly the iron overload in the whole liver. All of its components operate at room temperature. Since February 2005 about 150 patients and 90 healthy volunteers have been measured. The result of correlations with the LIC measurements by SQUID susceptometry in 43 patients showed R = 0.86. In 2 patients, affected by Hemochromatosis, we correlated the LIC measurement by MID with the assessment of the expected iron depletion obtained with the phlebotomy therapy (R =0.94). All the measurements were correlated with the serum-ferritin concentration values (R=0.72). We obtained correlation with the LIC measurement by liver biopsy in 7 patients (R = 0.89). The reproducibility of the iron overload of the same patients, measured after a relatively short lapse of time, is better than 0.5g. The data obtained shows that MID is a reliable instrument for the diagnosis of the liver iron overload and for the follow-up of the chelation therapy. It is simpler to operate being manageable directly in the Clinical Center and more affordable than competing techniques.
30 40 20 10 1 2 3 4 5 6 7 8 9 10 11 Accurate assessment of body-iron accumulation is essential for managing therapy of iron-overload in diseases such as thalassemia, hereditary hemochromatosis and other forms of severe congenital or acquired anemias. At present, the gold standard to determine liver-iron concentration (LIC) is the invasive liver needle biopsy; it might lead to large error in assessing iron burden due to the heterogeneous distribution of iron deposition in the liver. E. Butensky et al., Am J Clinical Pathology 2005; 123; 146-152 "Although chemical analysis of liver biopsy samples is considered the gold standard for determining the Liver Iron Concentration ..concern has been raised that variability in the distribution of liver iron deposition exists and might lead to errors as high as 200% in assessing body iron burden by biopsy." The distribution of the Liver Iron Concentration (LIC), obtained from the post-mortem examination of a thalassemic-patient liver, ranges from 10 (mg/g)* to 35 (mg/g)* LIC (mg/g)* * Dry weight
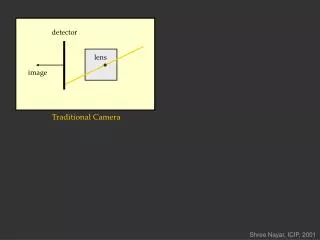
Pickup Magnet The magnetic field flux, threaded with the pickup, is slightly modified by the diamagnetic (mainly from water) and paramagnetic (iron) properties of tissues. It measures the iron overload in the whole liver
Pickup Magnet Pickup The symmetry, the mechanical stability and the accurate temperature control of the complete apparatusgivesthe sensitivity, better than 10-7, necessary to detect the iron quantity of interest. All the susceptometer components operate at room temperature Since February 2005, about 150 patients and 90 healthy volunteers have been measured.
Fiberglass supporting structure Thermal shield The signal of a smaller susceptometer, measuring rats, with and without the thermal shield. without with Inside the accessible region he magnetic field is lower than 1.9 10-2 T (CEI EN 60601-2-3, 1997-02)
x rail The stretcher moves on rails. We average a few differences between the signals, with the stretcher in and out of the sensitivity region, to account for the changes of the environment magnetic properties. This body position is to scan the liver region. Simply shifting the body allows measuring the magnetic signal of other body parts, for instance the head.
Because of ~100 nV error, the minimum quantity of detectable iron inside the entire liver region of the phantom is ~130 mg of Fe3+ or ~270 mg of iron with an effective magnetic moment of 4 Bohr Magneton. Small holes are evenly distributed on each of the phantom plastic slices.We poured paramagnetic powder, equivalent to 3g of Fe3+ and 15g of Fe3+, inside the holes placed in the phantom liver region. The signal picked up by the susceptometer has two sources: an overall magnetic background of the torso and a possiblecontribution from liver iron excess. After measuring the magnetic signature of a patient, statistical analysis methods and neural-network simulations (trained using the control data) are employed to estimate the background signal given the patient anthropometric data. Liver-iron overload is then determined by subtraction of the estimated background from the total measured signal.
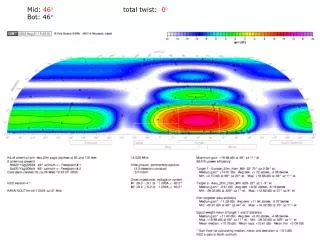
The signal of a patient, with 12.4±1 g of iron overload in the liver, is compared with the one of a healthy volunteer, having close anthropometric data. The abscissa x (cm) is the position of the center of the human body relative to the magnetic field axis.
y Magnetization signal x Eddy Current signal Magnetic flux from the body magnetization Magnetic flux from the body eddy currents EDDY CURRENT SIGNAL Because of the inductance of the eddy currents loops within the human body and the tissue resistivity, the delay of the eddy currents relative to the induced electric field isnegligible.
THE EDDY CURRENT SIGNAL DOES NOT DEPEND ON THE IRON • J. F. Schenck, E. A. Zimmerman, “Review Article High-field magnetic resonance imaging of brain iron: birth of a biomarker?,”N.M.R. Biomed, no. 17, pp. 433-445, 2004 “The concentration of iron in the tissues as free aqua ions is not significant” • In all the patient measurements we never noticed the iron overload skewness on the eddy current signal. The eddy current signal of the patient P029 is almost the same before and after the removal of his spleen, containing a large amount of iron. The eddy current signal of the patient P108, with more than 12g of liver iron overload, does not show any skewness
x 0 Both the eddy current and magnetization signals of a person without iron overload have a similar dependence on the body size. The estimation of the signal of the patient, supposed depleted by the iron overload (background signal), is based on his eddy current signal and anthropometric data.
Spleen: 14 slices mgFe/gdw 9.1 22.5 3.1 6.8 24.7 3.2 18.6 6.6 1.0 1.5 4.2 1.3 1.3 7.6 According with the chemical analysis of the cut off spleen (1350 g), the held iron was about 2.7g. Liver biopsy No iron overload in the liver The expected magnetization signal, obtained before the splenectomy, using the eddy current signal and the other patient's anthropometric data.
P 003 P 068 Measured (a) andBackground (b) signals of two patients affected by Congenital Hemocromatosis. The iron depletion is obtained with the phlebotomy therapy.
The iron reduction, measured by MID, is comparedwith the assessment of the iron depletion obtained with the phlebotomy therapy The iron overload measurements of the two Hemochromatosis patients
Measured (a) andBackground (b) signals of a Thalassemia Major patient, treated with 40mg/Kg of DFO 4 days per week and 75mg/Kg of Deferipron 7 days a week.
The MID sensitivity is about 1g (1SD). It depends on the model to calculate the background signal. The reproducibility of the iron overload of the same patients, measured after a relatively short lapse of time, is better than 0.5 g
Liver volume = (25cc/Kg) x (Patient’s body weight) (Ratio between dry-weight and wet-weight iron concentrations) = 5.83 The Liver Iron Concentration (LIC) of 7 patients from the MID and the Biopsy of their liver The LIC, measured by MID, is compared with the LIC measured by SQUID (Dr. A. Piga, Turin, Italy)on the same patients
The blood serum-ferritin reduction, of the two hemochromatosis patients, is compared with the reduction of the liver iron, measured by MID.
Comparison of the blood serum-ferritin variation with the measured variation of the iron in the liver of 27 patients, that have been measured at least twice by MID. MID Liver Iron Overload vs Blood Serum-ferritin Concentration