Download
1 / 65
660 likes | 678 Views
Explore the definition, pathophysiology, and management of liver disorders like hepatitis, including preventative measures, clinical manifestations, and nonsurgical and surgical treatment options.

E N D
Interventions for clients with liver, galdbladder and pancreas disorders. Clients with malnutrition and obesity. .
Liver disorders Hepatitis • 1. Definition: inflammation of the liver due to virus, exposure to alcohol, drugs, toxins; may be acute or chronic in nature • 2. Pathophysiology: metabolic functions and bile elimination functions of the liver are disrupted by the inflammation of the liver.
Hepatitis • Widespread viral inflammation of liver cells • Hepatitis A • Hepatitis B • Hepatitis C • Hepatitis D • Hepatitis E • Hepatitis F and G are uncommon
Hepatitis Viral Hepatitis • 1. Types (causative agents) a. Hepatitis A virus (HAV) Infectious hepatitis • 1. Transmission: fecal-oral route, often contaminated foods, water or direct contact, blood transfusions, contaminated equipment • 2. Contagious through stool up to 2 weeks before symptoms occur; abrupt onset • 3. Benign, self limited; symptoms last up to 2 months
Hepatitis • Prevention of Hepatitis A • Good handwashing • Good personal hygiene • Control and screening of food handlers • Passive immunization • Incubation period :20-50 days (short incubation period)
Hepatitis • Incidence • More common in fall and winter months • Usually found in children and young adults • Infectious for 3 weeks prior and 1 week after developing jaundice • Clinical recovery 3-16 weeks
Hepatitis Hepatitis B virus (HBV) • 1. Transmission: • infected blood and body fluids, • parenteral route with infusion • ingestion or inhalation of the blood of an infected person • Contaminated needles, syringes, dental instruments • Oral or sexual contact • High risk individuals include homosexual, IV drug abusers, persons with multiple sexual partners, medical workers • 2. Liver cells damaged by immune response; increased risk for primary liver cancer; causes acute and chronic hepatitis, fulminant hepatitis and carrier state
Hepatitis Hepatitis C virus (HCV) • 1. Transmission: infected blood and body fluids; injection drug use is primary factor • 2. Initial manifestations are mild, nonspecific • 3. Primary worldwide cause of chronic hepatitis, cirrhosis, liver cancer • 4. Usual incubation period 7-8 weeks
Hepatitis Hepatitis E virus (HEV) • 1. Transmission: fecal-oral route, contaminated water supplies in developing nations; rare in U.S. • 2. Affects young adults; fulminant in pregnant women
Clinical Manifestations • Abdominal pain • Changes in skin or eye color • Arthralgia (joint pain) • Myalgia (muscle pain) • Diarrhea/constipation • Fever • Lethargy • Malaise • Nausea/vomiting • Pruritus
Nonsurgical Management • Physical rest • Psychological rest • Diet therapy • Drug therapy includes: • Antiemetics • Antiviral medications • Immunomodulators
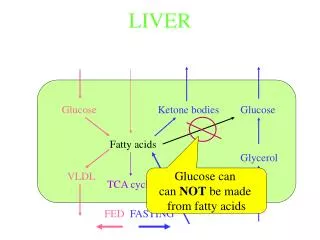
Fatty Liver (Steatohepatitis) • Fatty liver is caused by the accumulation of fats in and around the hepatic cells. • Causes include: • Diabetes mellitus • Obesity • Elevated lipid profile • Many clients are asymptomatic
Hepatic Abscess • Liver invaded by bacteria or protozoa causing abscess • Pyrogenic liver abscess; amebic hepatic abscess • Treatment usually involves: • Drainage with ultrasound guidance • Antibiotic therapy
Liver Trauma • The liver is the most common organ injured in clients with penetrating trauma of the abdomen, such as gunshot wounds and stab wounds. • Clinical manifestations include abdominal tenderness, distention, guarding, rigidity. • Treatment involves surgery, multiple blood products.
Cirrhosis • Cirrhosis is extensive scarring of the liver, usually caused by a chronic irreversible reaction to hepatic inflammation and necrosis. • Complications depend on the amount of damage sustained by the liver. • In compensated cirrhosis, liver has significant scarring but performs essential functions without causing significant symptoms.
Complications • Portal hypertension • Ascites • Bleeding esophageal varices • Coagulation defects • Jaundice • Portal-systemic encephalopathy with hepatic coma • Hepatorenal syndrome • Spontaneous bacterial peritonitis
Etiology • Known causes of liver disease include: • Alcohol • Viral hepatitis • Autoimmune hepatitis • Steatohepatitis • Drugs and toxins • Biliary disease • Metabolic/genetic causes • Cardiovascular disease
Clinical Manifestations • In early stages, signs of liver disease include: • Fatigue • Significant change in weight • Gastrointestinal symptoms • Abdominal pain and liver tenderness • Pruritus
Clinical Manifestations • In late stages, the signs vary: • Jaundice and icterus • Dry skin • Rashes • Petechiae, or ecchymoses (lesions) • Warm, bright red palms of the hands • Spider angiomas • Peripheral dependent edema of the extremities and sacrum
Abdominal Assessment • Massive ascites • Umbilicus protrusion • Caput medusae (dilated abdominal veins) • Hepatomegaly (liver enlargement
Other Physical Assessments • Assess nasogastric drainage, vomitus, and stool for presence of blood • Fetor hepaticus (breath odor) • Amenorrhea • Gynecomastia, testicular atrophy, impotence • Bruising, petechiae, enlarged spleen • Neurologic changes • Asterixis
Laboratory Assessment • Aminotransferase serum levels and lactate dehydrogenase may be elevated. • Alkaline phosphatase levels may increase. • Total serum bilirubin and urobilinogen levels may rise. • Total serum protein and albumin levels decrease.
Laboratory Assessment(Continued) • Prothrombin time prolonged; platelet count low • Decreased hemoglobin and hematocrit values and white blood cell count • Elevated ammonia levels • Serum creatinine level possibly elevated
Surgical Interventions • Peritoneovenous shunt • Portocaval shunt • Transjugular intrahepatic portosystemic shunt
Cancer of the Liver • One of the most common tumors in the world • Most common complaint: abdominal discomfort • Treatment includes: • Chemotherapy • Surgery
Liver Transplantation • Used in the treatment of end-stage liver disease, primary malignant neoplasm of the liver • Donor livers obtained primarily from trauma victims who have not had liver damage • Donor liver transported to the surgery center in a cooled saline solution that preserves the organ for up to 8 hours
Complications • Acute, chronic graft rejection • Infection • Hemorrhage • Hepatic artery thrombosis • Fluid and electrolyte imbalances • Pulmonary atelectasis • Acute renal failure • Psychological maladjustment
Acute Cholecystitis • Acute cholecystitis is the inflammation of the gallbladder. • Cholelithiasis (gallstones) usually accompanies cholecystitis. • Acalculous cholecystitis inflammation can occur in the absence of gallstones. • Calculous cholecystitis is the obstruction of the cystic duct by a stone, which creates an inflammatory response.
Chronic Cholecystitis • Repeated episodes of cystic duct obstruction result in chronic inflammation • Pancreatitis, cholangitis • Jaundice • Icterus • Obstructive jaundice • Pruritus
Clinical Manifestations • Flatulence, dyspepsia, eructation, anorexia, nausea and vomiting, abdominal pain • Biliary colic • Murphy’s sign • Blumberg’s sign • Rebound tenderness • Steatorrhea
Nonsurgical Management • Diet therapy: low-fat diet, fat-soluble vitamins, bile salts • Drug therapy: opioid analgesia with meperidine hydrochloride, antispasmodic or anticholinergic drugs, antiemetic • Percutaneous transhepatic biliary catheter insertion
Surgical Management • Laparoscopic cholecystectomy • Standard preoperative care • Operative procedure • Postoperative care • Free air pain result of carbon dioxide retention in the abdomen • Ambulation • Return to activities in 1 to 3 weeks
Traditional Cholecystectomy • Standard preoperative care • Operative procedure • Postoperative care • Meperidine hydrochloride via patient-controlled analgesia pump • Antiemetics • Wound care • Care of the T-tube • Nothing by mouth • Diet therapy
Cancer of the Gallbladder • Anorexia, weight loss, nausea, vomiting, general malaise, jaundice, hepatosplenomegaly, chronic, progressively severe epigastric or right upper quadrant pain • Poor prognosis • Surgery, radiation, chemotherapy
Acute Pancreatitis • Serious and possibly life-threatening inflammatory process of the pancreas • Necrotizing hemorrhagic pancreatitis • Lipolysis • Proteolysis • Necrosis of blood vessels • Inflammation • Theories of enzyme activation
Complications of Acute Pancreatitis • Hypovolemia • Hemorrhage • Acute renal failure • Paralytic ileus • Hypovolemic or septic shock • Pleural effusion, respiratory distress syndrome,pneumonia • Multisystem organ failure • Disseminated intravascular coagulation • Diabetes mellitus
Clinical Manifestations • Generalized jaundice • Cullen’s sign • Turner’s sign • Bowel sounds • Abdominal tenderness, rigidity, guarding • Pancreatic ascites • Significant changes in vital signs
Surgical Management • Preoperative care: NG tube may be inserted • Operative procedures • Postoperative care • Monitor drainage tubes and record output from drain. • Provide meticulous skin care and dressing changes. • Maintain skin integrity.
Chronic Pancreatitis • Progressive destructive disease of the pancreas, characterized by remissions and exacerbations • Nonsurgical management includes: • Drug therapy • Analgesic administration • Enzyme replacement • Insulin therapy • Diet therapy
Pancreatic Abscess • Most serious complication of pancreatitis; always fatal if untreated • High fever • Blood cultures • Drainage via the percutaneous method or laparoscopy • Antibiotic treatment alone does not resolve abscess
Pancreatic Carcinoma • Nonsurgical management • Drug therapy • Radiation therapy • Biliary stent insertion
Surgical Management • Preoperative care • NG tube may be inserted • TPN typically begun • Operative procedure may include Whipple procedure • Postoperative care • Observe for complications • Gastrointestinal drainage monitoring • Positioning • Fluid and electrolyte assessment • Glucose monitoring