Download
1 / 40
400 likes | 412 Views
Learn about the importance of timely newborn screening in Ontario and the results of a data-driven approach to determine safety in earlier screening. Discover how collecting samples at 24 hours of age could improve screening performance.

E N D
Changing the Time of Newborn Screen CollectionA Data-Driven and Safety-Oriented Approach Emeril Santander Michael Kowalski Laure Tessier Jennifer Milburn Pranesh Chakraborty
Objectives • Describe current sampling guidelines and the importance of timely screening in the context of Ontario’s universal newborn screening program • Describe results of a four-part approach taken to determine safety of earlier screening
Screening for Disease • Screening in general: • Detects treatable disease • Significantly speeding diagnosis & treatment • As early as possible • Prior to onset of severe or irreversible health outcomes • When delivery of treatment is most effective • As accurately as feasible • Screen Positives likely to be truly affected by disease • Screen Negatives likely to be unaffected by disease • A cost-effective way to identify elevated risk
Newborn Screening in Ontario Shortly After Birth A small sample of blood is taken
Newborn Screening in Ontario The sample of blood is dropped on to a special type of paper on the newborn screening card
Newborn Screening in Ontario Health care provider fills out information about the baby on the card, including datetime of birth and collection
Newborn Screening in Ontario The newborn screening sample is sent to Newborn Screening Ontario (NSO) in Ottawa for testing. Overnight courier service is used.
Newborn Screening in Ontario At the lab, several techniques are applied to evaluate for risk of metabolic, immune, endocrine, and other diseases. Up to 1200 samples per day
Newborn Screening in Ontario SCREEN POSITIVE PATIENTS SCREEN NEGATIVE PATIENTS Healthcare Provider Receives Negative Report • Are referred to specialist care at one of five regional treatment centres • Kingston General Hospital • Toronto Sick Kids • Ottawa Children’s Hospital • London Health Sciences • Hamilton Health Sciences • Diagnostic Testing • Healthcare Provider notified
Approximately 140 000 babies are born each year in Ontario ~1500 babies will screen positive ~ 250 babies will have a disease Working Against the Clock Aggressive Diseases: • Maple Syrup Urine Disease (MSUD) • Medium-Chain acyl-CoA dehydrogenase deficiency (MCADD) • Propionic Acidemia (PA) • MethylmalonicAcidemia (MMA) • Galactosemia (GALT) • Tyrosinemia (TYR) • Citrullinemia (CIT) • ASA Lyase Deficiency (ASA) • Congenital Adrenal Hyperplasia (CAH)
The Urgency of Detection Among the 250 infants detected each year truly affected by a screened disorder: 5% – 10% May die in the first week of life 10% – 20% Will be symptomatic in this first week Among the screened disorders, 20 of them have potential to cause irreversible harm in first two weeks of life
The Newborn Screening Sequence NSO now works 7 days per week New software tracks all packages en-route NSO refers critical patients on weekends BORN-supported electronic referral and diagnostic tracking
Timely Collection Timely Screen Historical Guideline 24 - 72 h after birth New Guideline 24 - 48 h after birth
Reviewing the literature – Methods and results 29 records identified from other sources 534 records identified in MEDLINE 5records after duplicates removed 558records screened 72 full-texts assessed 12full-texts included in literature review
Conclusions • No evidence that collecting dried bloodspot samples at 24 hours of age would increase NSO’s false-negative rate • Some evidence suggests that collecting samples at 24 hours of age would not increase the false-negative rate for PKU and CH (based on analyte values measured at 24 hours of age)
Finding Age Effects on Biomarkers The ideal observational study*: • Follow a large sample of newborns • With disease and without disease • Prick heel of each every hour • in the first 72 hours of life • Check for differences in biomarker levels by postnatal age • Determine if sampling age would change sensitivity or specificity of screening test * We can’t do this.
Finding Age Effects on Biomarkers Instead: • Retrospective Cohort • 553 newborns between 2010-2015 • Sampled more than once in first 72 hours of life ‘by chance’ No obvious reason for multi-sampling • Samples linked in system using demographics
Biomarker X Patient 1 HIGH Biomarker Value uL X at T1 X at T2 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
Biomarker X Patient 1 HIGH Biomarker Value uL X at T1 X at T2 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
Biomarker X Patient 1 … …. HIGH Patient 553 Biomarker Value uL 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
Biomarker X HIGH Biomarker X 72h trend Biomarker Value uL 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
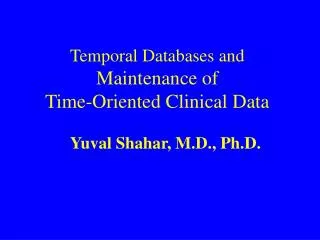
No Difference in Screening PerformanceWhen Trend is Stable Biomarker X HIGH Screen Positive Cutoff Values above this line are at elevated risk Biomarker Value uL 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
Increased Risk of False Positive Results When Trend is Negative Biomarker X HIGH Screen Positive Cutoff Values above this line are at elevated risk Biomarker Value uL 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
Increased Risk of False NegativesWith Upward Trend Biomarker X HIGH Screen Positive Cutoff Values above this line are at elevated risk Biomarker Value uL 0 0 24 hours 48 hours 72 hours Postnatal Age in Hours
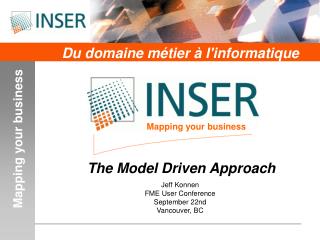
Thyroid Stimulating Hormone (TSH)Biomarker for Congenital Hypothyroidism(CH) False Positive True Negative True Positive
Thyroid Stimulating Hormone (TSH)Biomarker for Congenital Hypothyroidism(CH) False Positive True Negative True Positive
Postnatal TSH Elevation A well-known endocrine response to birth
Summary • Repeating this modelling across all screened biomarkers: • Certain endocrine markers will be elevated at an earlier age (false positive risk) • Potentially higher referral, recall, & diagnostics • Most trends were stable • No false negative risks identified
Background & goals Goal: Identify the impacts on screening performance caused by more samples being collected earlier Background: • 85% of samples in 2015 were collected 24-48 hours after birth • This number has grown by ~ 5%/yr since 2010 (…earlier discharges?) • There are no systematic individual differences in infants collected 24-48 hours vs. 48-72 hours.
Background & goals Key points (cont.): • Proportional indicators of screening performance in the 24-48h interval have remained stable, even as more samples are collected in this window • SPP24-48: 0.01% (screen positive rate) • SNR24-48: 99.99% (screen negative rate)
Method & Conclusion To forecast future performance we take the relevant proportions from the 24-48h interval and multiply them by the expected volumes of samples Conclusion: Most referrals will remain at current levels. Certain endocrine referrals may increase, although further optimization may be possible.
American Sampling Practices Research Question: Is this a common practice in other screening laboratories in North America? Method: Database review (NEWSteps) & survey Results: 93%of US jurisdictions collect newborn screening samples at 24-48 hours.
Summary & Conclusion New Guideline • Screening is time-sensitive • Reducing age at sampling is safe, we checked! • Certain false positives may occur, but work to mitigate these is ongoing • Screening at 24-48 hours is a widely-adopted practice in peer screening programs 24 - 48 h after birth