Download
1 / 49
490 likes | 523 Views
Learn about Endoscopic Submucosal Dissection (ESD) for colonic lesions, its techniques, instruments, and comparison with EMR. Discover indications, safety, complications, and treatment outcomes. Stay updated on the latest research and guidelines.

E N D
Current Status of Endoscopic Submucosal Dissection (ESD) for colonic lesions Surgical Grand Round 18.7.2015 HT Hung CMC
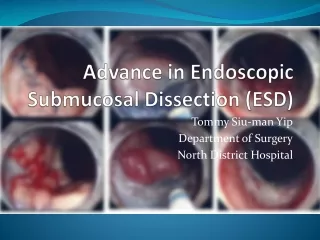
ESD Introduction • Endoscopic technique first developed by Hosokawa in 1998 for treating early gastric cancer • Shown to be highly effective and safe Tx • Later used for colorectal lesions • However… • longer length, narrower lumen, increase folds and thinner wall
Instruments / Devices • Water jet endoscope • Double-balloon CLN for precise control • Tip hood • Exerts tension on SM and aids easy entry • Bipolar needle knives • Electrosurgical current generator A: Jet B knife; B: IT knife nano; C: ST hood
Injection solution - hyaluronate • Facilitates good submucosal (SM) elevation • Indigo carmine for better visibility of the SM layer • CO2 insufflation • Rapid absorption, less distension / discomfort • Reduce risk of combustion when electrocautery is used
ESD vs EMR • EMR • Solution injected into submucosa of superficial type tumour • Lesion strangled with a snare and resected by high freq current Saito Y, Fukuzawa M, Matsuda T, Fukunaga S, Sakamoto T, Uraoka T et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surgical Endoscopy. 2010 Feb;24(2):343-52.
ESD • Solution injected into submucosa of tumour • The circumference of lesion incised with needle-type knife with electrical cutting current • SM then dissected • Can resect lesion in one piece (en bloc)
ESD Technique Zhou PH, Yao LQ, Qin XY. Endoscopic submucosal dissection for colorectal epithelial neoplasm. Surgical Endoscopy. 2009 Jul;23(7):1546-51.
Saito Y, Fukuzawa M, Matsuda T, Fukunaga S, Sakamoto T, Uraoka T et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surgical Endoscopy. 2010 Feb;24(2):343-52.
Update • ? Indication • ? Safety • ? Complication • ? Treatment outcome • recurrence, metastasis, prognosis • ? Follow up ???
Literature search from 1985 - 2012 • Evidence-based methods adopted but evidence scarce • Grades of recommendation by expert consensus • Level of evidence based on MINDS (Medical Information Network Distribution Service)
Excellent results obtained from both surgical and endoscopic Tx for colorectal ca • 5 yr survival rate 94% for stage 0 and 91% for stage 1 with surgery • Similar results for endoscopy (~93%) • However! • Patients’ age, co-morbidities, medication, life expectancy, etc
Indication for ESD – non-carcinoma • Resection recommended • adenoma 6mm • Superficial depressed-type lesions when 5mm • (Level of evidence IVb, Grade of recommendation B) • Carcinoma rate of protruded type and superficial elevated type lesions 5mm low • Rate of submucosal invasion as the size of the lesion IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
Indication for ESD - carcinoma • Endoscopic Tx for Early colorectal ca (Tis / T1a) • Little possibility of LN metastasis / deep invasion • Higher rate of cure with en bloc resection • Better path Dx of invasion depth x resection margin • (Level of evidence IVb, Grade of recommendation B) IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
In order to achieve R0, invasion depth (degree of submucosal invasion) precisely estimated with magnifying endoscopy, EUS, chromo-endoscopy before resection (ESD) • (Level of evidence IVb, Grade of recommendation B) • Lesion colour, surface unevenness, presence of depression, fold convergence etc IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
Biopsy avoided • May cause fibrosis in the submucosal layer -> non-lifting sign -> Endoscopic Tx will be difficult • (Level of evidence V, Grade of recommendation C1) • Recommend Dx based on magnifying endoscopic observation – more effective V: Descriptive study (case report and case series) C1: No scientific evidence exists but the therapy is recommended
Laterally spreading tumours (LST) • Macroscopic classification for mode of growth • Granular type (LST-G) • Homogenous (Homo) • Nodular mixed (Mix) • Non-granular type (LST-NG)* • Flat-elevated (F) • Pseudo-depressed (PD) • PD ass. w multifocal invasion and fibrosis
Subtypes of LST (indigo-carmine dye used) (a) LST-G Homo (b) LST-G Mix (c) LST-NG F (d) LST-NG PD
Indication for ESD for colorectal tumours Tanaka S, Kashida H, Saito Y, Yahagi N, Yamano H, Saito S et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Digestive Endoscopy. 2015 May 27(4):417-34
Complications • Perforation • Abdominal cavity is visible from colorectal lumen due to mural tissue defect • Rate 2-14% • Bleeding • No evidence based definition • Marked bloody stool, in Hb by >2 mg/dL, req blood transfusion etc • Rate 0.7-2.2%
Mx of perforation • When perforation occur, clipping should be done as far as possible regardless of location • (Level of evidence IVb, Grade of recommendation B) IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
When closure of perforation is complete, surgery can usually be avoided by giving antibiotics and fasting • Presence of free air on CT alone cannot be used to guide the decision for E-OT • E-OT is mandatory in case of incomplete closure of perforation
Mx of bleeding • Majority can be controlled by clipping, coagulation with ‘knife’ or haemostatic forceps • Severe bleeding seldom occurs in colon c.f. stomach in general • ? Preventive clipping – controversy • Pat should be hospitalised if necessary when delayed perforation or bleeding suspected • (Level of evidence IVb, Grade of recommendation B) IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
Assessment of Curability • Curability based on • Tumour margin of resected specimen • Risk factors for LN / distant metastasis • (Level of evidence IVb, Grade of recommendation B) IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
Tis (M) carcinoma • Generally do not met to LN / other organs • Can be radically cured by endoscopic local resection • Local recurrence reported with +ve lateral tumour margin • En bloc resection rate for ESD: • 84-94.5% (tumour 20mm)
T1 (SM) carcinoma • Radically cured when: • Vertical tumour margin –ve (histological complete resection) • Papillary or tubular adenocarcinoma • SM invasion depth < 1mm • No vascular invasion • Tumour budding grade 1 (low grade) • LN met and residual recurrence extremely rare • (Level of evidence IVb, Grade of recommendation B) IVb: Analytical epidemiological study: case-control study, cross sectional study B: Scientific evidence exists and the therapy is recommended
Post-op follow up • Aim: early detection of local residual / recurrence, metastasis and metachronous lesions • No evidence based consensus on the FU methods after endoscopic Tx • JSGE recommend FU CLN within 3 yrs • FU plan should be established with regard to techniques e.g. en bloc resection, curability evaluation based on pathology, risk factors for multiple lesions / carcinomas
Local residual / recurrence • Adenoma or pTis (M) carcinoma: No local residual / recurrence detected when complete en bloc resection achieved • pT1a (SM) carcinoma: Recurrence and met occurs even in cases where LN dissection performed • Recurrence rate in rectum (4.2-4.5%) is higher than in colon (1.5-1.9%)
Recurrence / metastasis occur mainly within 3-5 yrs for endoscopic Tx • Periodic FU req • Colonoscopy • Tumour markers (CEA) • US / CT
Metachronous lesions • After endoscopic Tx for T1 carcinoma: • Retrospective surveillance study showed metachronous lesions and early carcinoma detected in 54.8% & 11.9% of cases respectively • 3.4-26.5% of early colorectal ca, multiple metachronous carcinoma detected up to 102.8 months FU • Long term FU recommended
Risk of metachronous colorectal tumours high: • multiple (>3) colorectal adenomas with lesions >10mm in size • hx of colorectal carcinoma • Colonoscopy recommended 3 yrs after endo Tx • Multiple adenomas (>3) • Adenomas > 10mm in size • Villous adenomas • High grade dysplasia
Summary • ESD is a safe and reliable procedure to achieve en bloc resection of colorectal superficial neoplams when performed by experienced endoscopist who have acquired the necessary technical skills through adequate training • Adv: precise histopathological assessment, cure rate similar to conventional surgery • Disadv: difficult technique, steep learning curve, procedure may take long time, complications of perforation and bleeding, expensive
Important role in the Mx of colorectal tumours with improved safety and better devices in addition to skills and experience
Discussion Thank you
References • Tanaka S, Kashida H, Saito Y, Yahagi N, Yamano H, Saito S et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Digestive Endoscopy. 2015 May 27(4):417-34. • Sakamoto T, Mori G, Yamada M, Kinjo Y, So E, Abe S et al. Endoscopic submucosal dissection for colorectal neoplasms: A review. World Journal of Gastroenterology. 2014 Nov 21; 20(43): 16153–16158. • Sakamoto T, Takamaru H, Mori G, Yamada M, Kinjo Y, So E et al. Endoscopic submucosal dissection for colorectal neoplasms. Annals of Translational Medicine. 2014; 2(3)26.
Saito Y, Fukuzawa M, Matsuda T, Fukunaga S, Sakamoto T, Uraoka T et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surgical Endoscopy. 2010 Feb;24(2):343-52. • Zhou PH, Yao LQ, Qin XY. Endoscopic submucosal dissection for colorectal epithelial neoplasm. Surgical Endoscopy. 2009 Jul;23(7):1546-51.
Tanaka S, Oka S, Chayama K. Colorectal endoscopic submucosal dissection: present status and future perspective, including its differentiation from endoscopic mucosal resection. Journal of Gastroenterology. 2008;43(9):641-51. • Tamegai Y, Saito Y, Masaki N, Hinohara C, Oshima T, Kogure E, et al. Endoscopic submucosal dissection: a safe technique for colorectal tumors. Endoscopy. 2007 May;39(5):418-22.
Repici A, Hassan C, De Paula Pessoa D, Pagano N, Arezzo A, Zullo A, et al. Efficacy and safety of endoscopic submucosal dissection for colorectal neoplasia: a systematic review. Endoscopy. 2012 Feb;44(2):137-50. • Yamamoto H. Endoscopic submucosal dissection for colorectal tumors. Interventional and Therapeutic Gastrointestinal Endoscopy. Front Gastrointest Res. Basel, Karger, 2010, vol 27, pp 287–295.
NICE Guideline 2010 for ESD • Systemic review of 14 studies and 1314 patients • En bloc resection rate 85% • Complete cure 75% (en bloc resection with histologically clear margin)
Review article in Endoscopy 2012 22 studies from 1999-2010 (20 Asian, 2 European), on 2841 ESD-treated lesions Repici A, Hassan C, De Paula Pessoa D, Pagano N, Arezzo A, Zullo A, et al. Efficacy and safety of endoscopic submucosal dissection for colorectal neoplasia: a systematic review. Endoscopy. 2012 Feb;44(2):137-50.
22 studies from 1999-2010 (20 Asian, 2 European), on 2841 ESD-treated lesions Repici A, Hassan C, De Paula Pessoa D, Pagano N, Arezzo A, Zullo A, et al. Efficacy and safety of endoscopic submucosal dissection for colorectal neoplasia: a systematic review. Endoscopy. 2012 Feb;44(2):137-50.
Repici A, Hassan C, De Paula Pessoa D, Pagano N, Arezzo A, Zullo A, et al. Efficacy and safety of endoscopic submucosal dissection for colorectal neoplasia: a systematic review. Endoscopy. 2012 Feb;44(2):137-50.
FU data after ESD Repici A, Hassan C, De Paula Pessoa D, Pagano N, Arezzo A, Zullo A, et al. Efficacy and safety of endoscopic submucosal dissection for colorectal neoplasia: a systematic review. Endoscopy. 2012 Feb;44(2):137-50.
Kudo’s classification for pit pattern • Based on pit pattern of colonic mucosa • 5 types • Type I to V • Type III has subtypes III-S and III-L • Type I & II are benign, type III to V are malignant
Images show type V1 pit patterns after crystal violet staining. The morphological pattern of a low-grade type V1 pit pattern lesion (a) is less irregular and destructive than that seen in lesions with a high-grade type V1 pattern (b) A type VN (non-structural) pit pattern corresponds to a high degree of submucosal cancer invasion
Tamegai Y, Saito Y, Masaki N, Hinohara C, Oshima T, Kogure E, et al. Endoscopic submucosal dissection: a safe technique for colorectal tumors. Endoscopy. 2007 May;39(5):418-22.
Classification of early colorectal neoplasms according to the Japanese Society for Cancer of the Colon and Rectum