Download
1 / 38
380 likes | 395 Views
Explore the intricate network of endocrine cells in the GI tract and pancreas, their functions and clinical implications. Learn about important hormones such as gastrin, secretin, and CCK, as well as tumors like insulinomas and gastrinomas.

E N D
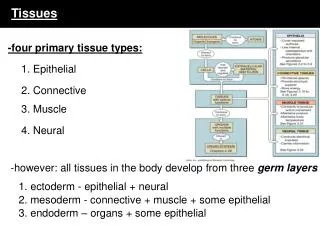
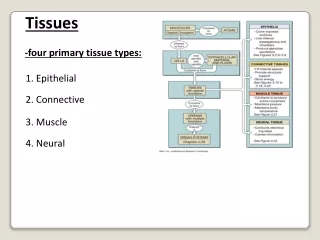
Endocrine tissues • Pituitary gland/hypothalamus • Thyroid gland • Parathyroid glands (4) • Adrenal glands (2) • Ovaries (2) • Testes (2) • GI/Pancreatic Endocrine System
Endocrine cells of the GI tract are scattered (not in discrete glands)
Gastric D (somatostatin) cells Immunofluorescence (SLI) Immunohistochemistry (SLI)
Gastric ECL (enterochromaffin like) cells Silver stain of gastric mucosa ECL cells are argyrophilic; they produce histamine.
Endocrine Cells of the Stomach PROXIMAL DISTAL
Gastric G (gastrin) cells Immunohistochemistry (gastrin)
Pancreatic endocrine cells are concentrated in islets scattered through the organ α: Glucagon β: Insulin δ: Somatostatin
(e.g., gastrin, secretin) (e.g., somatostatin, histamine)
Physiology of selected GI hormones (Endocrine actions) Gastrin: ↑ gastric acid secretion (target: ECL cell) Secretin: ↑ pancreatic HCO3- secretion (target: duct cell) CCK: ↑ pancreatic enzyme secretion and gallbladder contraction (target: neurons with CCK receptors) GIP, GLP-1 (incretins): ↑ glucose-mediated insulin secretion, improving oral glucose tolerance (target: β cells) GLP-2: stimulates growth of intestinal epithelial cells (target: intestinal stem cells?)
Gastrin-17 is a hormone controlling gastric acid in humans. Feldman et al, J. Clin Invest 1977 *
Negative Feedback Loop Food Gastrin Acid + + ↑Protonation of AAs ↑Somatotostatin (antrum) ↑Secretin (duodenum)
Clinical Corollary: Gastric Carcinoid Pernicious anemia/chronic atrophic gastritis, with chronic achlorhydria/hypochlohydria (low acid)→ Loss of negative feedback of acid on gastrin Chronic, persistent hypergastrinemia → ECL cell hyperplasia → Increased risk of Type 1 gastric carcinoid tumors (carcinoidosis)
Negative Feedback Loop Food + + CCK Pancreatic trypsin ↓CCK-RF (duodenum) ↓Monitor peptide (pancreas)
Clinical Corollary: Chronic Pancreatitis • Pancreatic insufficiency (low trypsin) • Chronically high plasma CCK → • Chronic pancreatic stimulation→ • Chronic pain • Therapy: Pancreatic enzymes between and with meals • Trypsin digests CCK-RF and monitor peptide • Lowers plasma CCK levels • Less pancreatic stimulation • Less pain
Products of GI/Pancreatic Endocrine Cells Polypeptides (N>30) • Half-lives usually in minutes (e.g., somatostatin, insulin, G-17) • Peptide analogs (agonists) may have half lives of hours (e.g., octreotide, insulin analogs) • Peptide antagonists are difficult to develop
Products of GI/Pancreatic Endocrine Cells Non-Peptide Products • Half-lives usually in seconds • Analogs (agonists) may have half lives of hours • Antagonists are easier to develop and in common use AMINE PRODUCTSHistamine, 5-HT, GABA, Dopamine,Norepinephrine, Epinephrine NON-AMINE PRODUCTS Acetylcholine (cholinergic), ATP (purinergic), Nitric oxide (nitrergic)
Amine Precursor Uptake and Decarboxylation EC cell ECL cell Chromaffin cell Tyrosine Histidine (AP) Tryptophan + OH + OH DOPA 5-OH Tryptophan dopamine Rs histamine Rs norepi Rs 5-HT (serotonin) Rs Rs epi Rs,receptors
Excessive amine production by NETs • Chromaffin cells (stain with chromium salts) • Adrenal medulla and sympathetic ganglia • Amine Products: epinephrine, norepinephrine, dopamine • Tumors: pheochromocytoma • Enterochromaffin (EC) cell (stain with chromium salts) • GI mucosal endocrine cells (also stain with silver salts) • Amine Product: 5-hydroxytryptamine (5-HT; serotonin) • Tumors: carcinoids (NETs) carcinoid syndrome • Enterochromaffin-like (ECL) cell • Gastric/ bronchial mucosal endocrine cells (stain with silver salts) • Amine Product: histamine • Tumors: carcinoids (NETs) atypical carcinoid syndrome
Insulinoma • Annual Incidence: 1-2/million • Pancreatic >>>> Nonpancreatic • Incidence of malignancy: <10% • Incidence in MEN-1: 18% (7%-31%) • Clinical Features: fasting hypoglycemia • Neuroglycopenic symptoms (e.g., visual, confusional) • Adrenergic symptoms (e.g., sweating, tremulousness)
Insulinoma in a patient with MEN-I and fasting hyperinsulinemic hypoglycemia
Gastrinoma (ZE Syndrome) • Annual incidence: 0.5-1.5/million • Duodenum > Pancreas >>> other • Incidence of malignancy: 60%-90% • Incidence in MEN-1: 54% (20%-61%) • Clinical Features: • Abdominal pain/ Peptic Ulcer Disease, often with GI bleeding • GI perforation: 5% • Diarrhea/ Steatorrhea • GERD • Esophageal stricture: 4% • Nausea/Vomiting • MEN-1: 22%
Gastrinoma: Pathology Pancreas 2-3 cm Duodenum
VIPoma(Verner-Morrison; WDHA; Pancreatic cholera) • Annual incidence: 0.05-0.2/million • Pancreatic > nonpancreatic in adults (intestinal, bronchial, pheo) • Ganglioneuroma or ganglioneuroblatoma in young kids (< age 10) • Incidence of malignancy: > 60% in adults • 10% in young kids and rare adults with this tumor • Incidence in MEN-1: 1% (1%-12%) • Clinical Features: • Secretory diarrhea • Volume depletion • Weight loss • Abdominal cramps, colic • Flushing • Hypokalemia,Hypochlorhydria, Hypercalcemia, Hyperglycemia
Glucagonoma • Annual incidence: 0.01-0.1/million • Pancreatic >> non-pancreatic • Incidence of malignancy: 50%-80% • Incidence in MEN-1: 3% (1%-6%) • Clinical Features: • Dermatitis (NME) • Diabetes/glucose intolerance • Weight loss • Glossitis/cheilitis/stomatitis • Diarrhea • Abdominal pain • VTE • Hypoaminoacidemia • Hypocholesterolemia
Somatostatinoma • Annual incidence: very rare • Pancreatic> Duodenal>> other sites • Incidence of Malignancy: > 70% • Incidence in MEN-1: <1% • Clinical Features (can be due to tumor per se or ectopic production of somatostatin) • Diabetes mellitus • Gallbladder disease • Diarrhea/steatorrhea • Weight loss
GH-RFoma (GRFoma) • Annual incidence: very rare • Lung> Pancreas > Small Intestine> Other sites • Incidence of malignancy: > 30% • Incidence in MEN-1: < 1% • Clinical Features: • Acromegaly due to ectopic production of GH-RF • GH and somatomedin-A levels elevated • Pituitary enlargement MEN-1
Other Reported Functional NETs (?significance) • ACTHoma • may occur with gastrinoma • CCKoma • Neurotensinoma • Erythropoietinoma with polycythemia • LHoma with masculinization (F) or loss of libido (M) • Reninoma with hypertension • PTHrPoma with hypercalcemia
Carcinoid tumors (GI-NETs) • MORE COMMON • Small intestinal (ileal, duodenal, jejunal) • Gastric (Types 1-3) • 1: achlorhydric • 2: Gastrinoma with MEN-1 • 3. Sporadic • Bronchial/Pulmonary • LESS COMMON • Appendiceal • Rectal • Colonic • Esophageal • Pancreatic
Carcinoid syndrome • Occurs when sufficient concentration of hormonal products (amines and polypeptides) released by the tumor enter the systemic circulation. • Occurrence of carcinoid syndrome, and its severity, are related to the tumor size in areas that drain into the systemic circulation. • Hepatic veins (in liver mets), the most common (>90%) • Ovarian/Testicular veins (in gonadal carcinoids) • Pulmonary veins (in bronchopulmonary carcinoids) • Retroperitoneal veins (in GI/pancreatic tumors with local spread)
Clinical Features: Carcinoid Syndrome • Flushing: 70-80% (probably from tachykinins [SP,NKA, etc.] • Diarrhea: 70-80% (probably from 5-HT in many patients) • Carcinoid valvular heart disease: 26-30% • R>>L heart; probably from 5-HT in most patients • Wheezing/asthma: 11-12% (probably from 5-HT/histamine) • Pellagra: 1-2% (from diversion of dietary niacin to 5-HT synthesis, leading to niacin deficiency)
Somatostatin and GI-Carcinoid/pNETs • Many GI carcinoids/pNETs expressreceptors for somatostatin. • Such somatostatin receptors can be used in the diagnosis & therapy of patients with carcinoids/NETS, using radiolabeled analogs of somatostatin, such as octreotide and lanreotide. • When GI endocrine tumors produce somatostatin, they are called somatostatinomas. • Somatostatinomas may or may not cause the somatostatinoma syndrome (diarrhea, steatorrhea, diabetes, and gallstones). This humoral syndrome has been questioned. Octreotide scans. Note uptake in bladder, kidneys, and spleen, and metastases to the liver and to para-aortic nodes (arrows).
PPomas and Nonfunctional (NF) pNETS • PPomas (no clinical syndrome) • NF-pNETs • Present as asymptomatic lesions detected by imaging • Present as mass lesions with local symptoms • Presentation similar to pancreatic adenocarcinoma • Stain + for chromogranin A and neuron specific enolase
Approach to a Patient with a GI or Pancreatic NET • Step 1: Is the Tumor Functional? • Clinical assessment • Measurement of plasma/urinary hormones, amines or metabolites • Control hormonal hypersecretion if present and possible to prevent morbidity and mortality • Step 2: Tumor Localization and Staging (TMN) • CT/MRI, Endoscopy/EUS±FNA, Somatostatin Receptor Scintigraphy • Hepatic vein sampling after intra-arterial calcium or secretin in hard-to- localize, functional tumors 7 mm gastrinoma in head of pancreas
Therapeutic Approach to NETS • Surgery is the only curative option, but may have adverse effects (e.g., Whipple for small, well-differentiated, G1 pNET) • Incidentalomas without hormonal overproduction and local symptoms: • role of watchful waiting ,especially in higher risk surgery patients • Metastases-directed therapies may reduce tumor burden and prolong survival and quality of life, but have adverse effects • Hepatic embolization • Hepatic chemoembolization • Radionuclide receptor targeted therapy (somatostatin analogs) • Systemic chemotherapy with mTOR inhibitors, interferon, or cytotoxic agents in patients with advanced disease
GI-NETs and pNETS • Sporadic tumors (more common) • Autosomal dominant inherited syndromes • MEN-1 • Tuberous sclerosis • NF-1 • VHL
Inherited Syndromes: GI-NETs and pNETs NF, nonfunctional