Download
1 / 28
300 likes | 442 Views
Explore the historical milestones of Civilian Tactical EMS, the birth of Civilian EMS in the 1860s, and the emergence of SWAT teams shaping Tactical EMS. Discover the evolution of medical support in civilian tactical operations and the roles of Team Medics in ensuring mission success and safety.

E N D
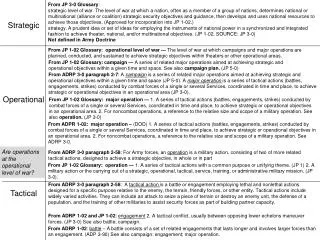
Civil Sector Tactical EMS Jeffery C. Metzger, M.D. Tactical Physician, Dallas Police Department Fellow, Government Emergency Medical Security Services Assistant Professor, University of Texas, Southwestern Medical Center Deputy Medical Director, Biotel Systems
Objectives • Background of Civilian TEMS • Current Models and Practice • Differences between Civilian and Military Medical Support • Case Review
In the beginning… • Initially left until the battle was over • Early 1700s, Napoleon Bonaparte appointed Dominique-Jean Larrey to develop patient care program • Mid-1800s during U.S. Civil War Dr Jonathan Letterman refined Larrey’s concepts and developed horse-drawn ambulance chains • Also during Civil War, Clara Barton developed the practice to “treat them where they lie.” "The remoteness of our ambulances deprived the wounded of the requisite attention,“ Dominique-Jean Larrey
Birth of Civilian EMS • 1865 – Cincinnati General Hospital • Grady Hospital in Atlanta • Charity Hospital in New Orleans • Free Hospital of New York (Bellevue) • Funeral Home Service
Without SWAT, there would be no TEMS • August 1965 – Watts Riots • 34 people killed, 1,100 people injured, 4,000 people arrested, 600 buildings damaged or destroyed, and an estimated $35 million in damage
Without SWAT, there would be no TEMS • August 1st, 1966, University of Texas at Austin • Charles Whitman climbs to the top of the campus clock tower and kills 15 people and wounds another 31 others
Emergence of S.W.A.T. • 1967 - Los Angeles Police Department • Officer John Nelson and Inspector Daryl Gates • “The purpose of SWAT is to provide protection, support, security, firepower, and rescue to police operations in high personal risk situations where specialized tactics are necessary to minimize casualties.”
A Fledgling Sub-Specialty 1980’s - Many departments begin to train their own officers in basic first aid and trauma care, or train paramedics and EMTs in law-enforcement tactics 1989 and 1990 – The first national conferences bring together experience and expertise from more than 40 tactical agencies 1990 – Casualty Care Research Center develops a database to catalogue injuries sustained by law enforcement officers and (with DoD, DoI, US Park Police, and Uniformed Services University) develops the Counter Narcotics and Terrorism Operational Medical Support (CONTOMS) course
Gaining Support 1993 – California Chapter of ACEP organized the Subcommittee on Tactical Emergency Medicine 1993 – National Tactical Officer Association published a position paper supporting specialized medical support for tactical operations. 1999 – National Association of EMS Physicians formed a task force to look at issues surrounding TEMS and published their supportive position paper in 2001
Variations on a Theme Officer with first aid training Officer trained as EMT Practicing EMT Practicing paramedic Practicing physician Note: Not To Scale
Goals of Civilian Medical Support • Keep the team operating at peak operational performance and to increase the possibility of mission success while decreasing the risk to the officers, suspects, and bystanders
Role of the Team Medic • Preventative medicine • Ensuring the physical and emotional health of the team • Vaccinations (hepatitis, tetanus) • Training officers in self- and buddy-aid • Education (diet strategies/supplements, hydration, routine health maintenance)
Role of the Team Medic • Training Exercises • A significant number if injuries occur during training exercises • Training with the team will allow the team to learn the medics abilities and the medic to learn tactics and how to integrate with the team
Role of the Team Medic • Pre-operational planning • Medical Threat Assessment • Heat/cold illness, dehydration, hazardous chemicals, plant threats, structural issues, planned evac routes, etc • Equipment selection
Medical Care During the Mission • Care Under Fire • Tactical Field Care • Combat Casualty Evacuation Care • Medicine Across the Barricade • Tactical Team, Bystanders, Suspects • K9 care
Preservation of evidence • In most instances, especially those involving injuries, the entire environment is a crime scene • The medic must perform the necessary medical care while making every attempt to preserve evidence
Screening Prior to Incarceration • Evaluation and treatment on scene may prevent the need to transport a suspect to a medical facility, decreasing the associated costs and risks • Must know local policies and guidelines, as well as medical capabilities available at the detention facility
Medical Liability • Depends on the level of the provider, • Medics must operate under a medical director, and are limited to the agency’s SOPs unless changed by the medical director • Physicians may or may not be covered under their hospital’s liability policy
Major Differences in Civilian vs Military Tactical Medicine • Tactical considerations • Weapons used • Extended • Gear • Mission Objective • Patient number • Location security • Supplies and advice • Environment • Prehospital phase • Communication • Transport – time /capability
Case Review • Disclaimer: This incident is still under investigation and what is presented is my personal observations and understanding of the events as they transpired.
Case Review • February 16th, 2006 • Dallas Police SWAT team was asked by the DEA’s Dallas Division to execute a knock-and-announce search warrant on Alejandro Tamayo at 1228 Oak Park in Dallas
Case Review • During the search, law enforcement officers seized approximately $130,000 in U.S. currency, eight firearms and approximately two kilograms of cocaine.
Follow-up • A federal indictment released April 7th 2006 charges ringleader Alejandro Tamayo, age 44, with one count of conspiracy to distribute methamphetamine, one count of possession with intent to distribute cocaine, one count of possession of a firearm during and in relation to a drug trafficking crime, one count of possession of a firearm during and in relation to a crime of violence and two counts of assault on a federal officer. If convicted Tamayo faces a minimum of 10 years imprisonment and a maximum of life imprisonment without parole. Tamayo is presumed innocent until proven guilty.
Contact Information Jeffery C. Metzger, M.D. Mail Code 8890 5323 Harry Hines Blvd. Dallas TX, 75390-8890 cell (972)322-2225 jeffery.metzger@utsw.edu