Download
1 / 7
80 likes | 247 Views
Glycemic Control in Type 2 Diabetes: How Tight is Too Tight?. Frederick L. Brancati, MD, MHS Professor of Medicine & Epidemiology Director, Division of General Internal Medicine Visit Hopkins GIM at www.hopkinsmedicine.org/gim. NCH Healthcare System, Naples, FL 21 January 2010.

E N D
Glycemic Control in Type 2 Diabetes: How Tight is Too Tight? Frederick L. Brancati, MD, MHS Professor of Medicine & Epidemiology Director, Division of General Internal Medicine Visit Hopkins GIM at www.hopkinsmedicine.org/gim NCH Healthcare System, Naples, FL 21 January 2010
Objectives • Identify controversy in diabetes care • Establish framework for decision-making • Compare/contrast results from recent trials
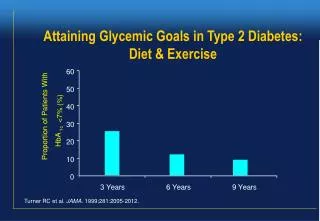
Why Treat A1c to 7% Target ? • Hyperglycemia predicts micro & macrovascular disease epidemiologically • The link with micro & macrovascular disease is biologically plausible • Hyperglycemia poses non-vascular risks • Infection, Hypovolemia, Urinary Frequency • Improved glycemic control reduces risk of microvascular disease
Why Treat A1c to 7% Target ? • Improved glycemic control reduces CVD in • Type 1 diabetes (DCCT) • Recently diagnosed type 2 diabetes (UKPDS) • Black box warnings require context • Lactic acidosis with metformin is very rare • CHF with TZDs is relatively mild/reversible • Black box MI warning for rosiglitazone only
Cumulative Risk of Infectious Disease Death by Diabetes Status in US Adults, NHANESII Mortality Study AG Bertoni et al. Diabetes Care 2001 24:1044-9.
Age, Sex, Race-Adjusted Relative Hazard of CHD by HbA1c in 1321 Adults without Diabetes (A) and 1626 Adults with Diabetes (B) Selvin, E. et al. Arch Intern Med 2005;165:1910-1916.
Cumulative Incidence of First Episode of Falling in 139 Elderly Nursing Home Residents by Diabetes Status In multivariate analysis, only diabetes (adjusted hazard ratio 4.03; 95% confidence interval, 1.96–8.28) and gait and balance (adjusted hazard ratio 5.26; 95% confidence interval, 1.26–22.02) were significantly and independently associated with an increased risk of falls. MS Maurer et al. J Gerontol A Biol Sci Med Sci (2005) 60:1157–62