Download
1 / 15
150 likes | 271 Views
Chronic Leukemias. C L L. C M L. CML. A clonal disease results from an acquired genetic change in a pluri-potential hemopoietic stem cell within the BM. The altered stem cell proliferates and generates a population of differentiated cells that gradually replace normal hemopoiesis.

E N D
C L L C M L
CML A clonal disease results from an acquired genetic change in a pluri-potential hemopoietic stem cell within the BM. The altered stem cell proliferates and generates a population of differentiated cells that gradually replace normal hemopoiesis.
CML The disease is bi-phasic or tri-phasic with a: i) A chronic phase ii) An acute phase, and iii) Sometimes an intervening accelerated phase.
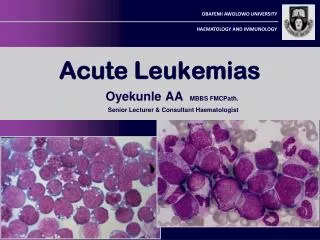
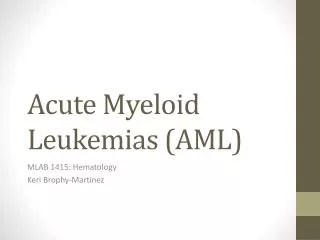
The characteristic findings in CML ►Laboratory CML: usually diagnosed in the initial chronic “indolent” phase. The WBC count at diagnosis is usually in the range 20-200 ×109/L Occasionally, patients may present with leukocyte numbers in the range 200-800 ×109/L. a) PB: The blood film shows a full spectrum of cells in the granulocyte series, FROM “blast cells TO mature neutrophils” BUT intermediate myelocytes and neutrophils predominate. b) BM Hypercellular marrow, increased M:E ratio. ►Clinical: anemia is usual and huge splenomegaly is frequently seen.
The peripheral blood film in patients with CML, may show VARING cells as: promyelocytes (P) myelocyte (M) eosinophil (E) basophil (B) (NUMEROUS) neutrophils (N) band forms (BF)
P M N E P B BF BF BF A peripheral blood film in a patient with (CML) diagnosis
The fusion gene BCR-ABL, that was originally detected by cytogenetics studies, today is routinely used in CML in most centers around the world (BUT NOT HERE). Found in >95% of CML cases
CLL As the disease state is mostly silent and with an insidious onset, incidental diagnosis now occurs in 70-80% of patients. CLL is a chronic B-lineage lymphoproliferative disorder (LPD) defined by characteristic morphology and immunophenotyping findings. The cell of origin in CLL is now thought to be: an activate B-cell that has undergone somatic hypermutation of IGVH genes. Much common in the western hemisphere than us.
How to Diagnose CLL? • a lymphocyte count of at least 5 ×109/L (5,000 cells per cubic mm) was sufficient for diagnosis when: • The immunophenotype was typical (CD19+/CD5+). • B-cell clonality was demonstrated (Monoclonal B-cell lymphocytosis) • the proliferated cells express either Kappa or LambdaBUT NOT BOTH.
Hairy Cell Leukemia It is always associated with splenomegaly, which tends to progress slowly. Lymph node enlargement is usually absent. BM aspirates are unsuccessful as no fragments and few cells are obtained. ►Trephine BM biopsy is essential. ►Most cases present hematologically with: leukopenia, neutropenia, and typically with monocytopenia. It usually affects males THAN female and above age 40. Splenomegaly, Hepatomegaly, Pancytopenia, Hairy lymphocytes
How to Diagnose Hairy Cell Leukemia The recognition of typical hairy cells in PB films is useful for suggesting this diagnosis. Hairy cells are large, twice the size of a normal lymphocyte, and have abundant cytoplasm, that is characteristically villous in its outline
Tartrate-resistant acid phosphatase (TRAP) demonstrated on hairy cells corresponds to a unique isoenzyme and is specific for HCL. This enzyme can be used in BM biopsy. Tartrate-resistant acid phosphatase (TRAP) activity in three hairy cells