Download
1 / 24
250 likes | 627 Views
Leukemias . Etiology of Leukemias General outlines Acute leukemias Single cell mutation with “freezing” farther cell’s differentiation and maturation in early stages of development (e.g. stem cell) Chronic leukemias

E N D
Etiology of Leukemias General outlines Acute leukemias Single cell mutation with “freezing” farther cell’s differentiation and maturation in early stages of development (e.g. stem cell) Chronic leukemias The abnormal mutated (or transformed) cells will retain some capabilities to maturate (and differentiate) beyond the early cells (blasts) BUT they are all abnormal and useless malignant cells.
A systematic approach to diagnose different hematologic neoplasms: • 1) CBC (Complete Blood Count), CBP (Complete Blood Picture) • a) WBC total, differential count, left shift?, • b) Peripheral blood film: evaluate the cellular constituents and search for abnormalities (abnormal cells?). • 2) Special staining (SBB, MPO, NSE, etc). • 3) Bone marrow aspiration: • assess the cellularity • M:E ratio • percentage of blast cells • The maturation and differentiation of various cell lineage (Lymphoid, Myeloid). • 4) Bone marrow biopsy (trephine biopsy): • ► in solid tumors (as lymphomas with invasion to Bone marrow) • ► in cases that Bone marrow aspiration not possible (AML-M7 “due to fibrosis”, Hairy cell Leukemias, etc) • ► in cases with a compact bone marrow “very high cellular proliferation and a dry tap” • 5) Immunophenotyping: • Use of cell surface, cytoplasmic, or nuclear markers to define cell’s character and origin (phenotyping) BY • Flow cytometry and Immunohistochemistry studies. • 6) Genetics studies • ► Cytogenetics findings • ► Molecular genetics studies
Leukemia classification • ►1976 • French, American and British hematologists (FAB group) proposed • a classification system (FAB classification): • Morphologic assessment • Special staining techniques (if required) • Limited use of Monoclonal antibodies (in selected cases) • ► 2001 • WHO classification of Hematopoietic and Lymphoid malignancies. • i) Adopting the FAB morphologic classification. • ii) Limited use of special staining techniques. • iii) Wider use of immunophenotyping (cell markers) studies (FC, IHC) • iv) Cytogentics and Molecular genetics studies used heavily to define • v) The character and prognosis of various disease entities. • ► 2008 • An Updated WHO classification has been edited.
Differences between FAB and WHO • FAB-classification: • Heavily used “Morphologic Findings” • Special staining (SBB, MPO, NSE, etc), if required • WHO-classification: • Morphologic findings • Special staining (decreased role) • Immunophenotyping (in the form of FC and IHC) heavily used. • Cytogentics and Molecular genetics studies frequently used.
Leukemias Acute leukemias Chronic leukemias Lymphoid Myeloid L1 L2 L3 M0 M1 M2 M3 M4 M5 M6 M7 The original FAB-Classification system of Acute Leukemias, heavily based on morphologic findings
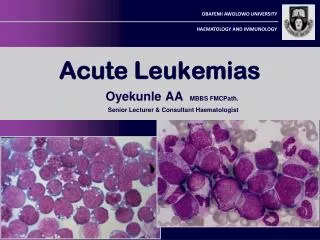
L3 L1 L2 Myeloblast type I Myeloblast type II Types of blast cells in ALL and AML
FAB-classification of ALL L1-lymphoblasts in the BM ALL-L1 L2-lymphobalsts in the BM ALL-L2 ALL-L3 L3-lymphoblasts in the BM SBB (SHOULD BE –ve) MPO (SHOULD BE –ve)
FAB-classification of AML M0 Undifferentiated blast cells (Myeloid origin by immunophenotyping), Special staining SBB-ve, MPO-ve M1 Myeloblasts (≥ 20% in BM) SBB+ve, MPO+ve M2 Myeloblasts (≥20% in BM) SBB+ve, MPO+ve M3 Abnormal Promyelocytes SBB+ve, MPO+ve M4 Myeloblasts (20-80%) + Monocytes (>20%), NSE +ve M5(a): Monoblasts ≥80% NSE +ve (b): Monoblasts <80%, more promonocytes and monocytes in BM,NSE +ve M6 Erythroleukemia, 50% of BM cells are of erythroid lineage M7 Blast cells are ≥20% of BM cells (they are identifiable as Megakaryoblasts).
2 important Practical points: • BM aspiration results in acute leukemia, although may be: • i) dry tap or • ii) difficult to aspirate (hypercellular marrow with excessive marrow blasts) • BUT is never ever an empty marrow. • Leukemoid reaction should be distinguished from Leukemias “of particular CML” • Neutrophil Alkaline Phosphatase Score • C-reactive protein, ESR, and other inflammatory indicators. • Blood film finding (left shift). • Bone marrow aspiration, Bone marrow biopsy, immunophenotyping • and cytogentics studies may required accordingly.
The Current WHO classification has widely used the immunophenotyping to characterize leukemias and lymphomas Frequently used Immunophenotyping & Genetics studies
The Panel of Antibodies recommended by the British Committee for Standards in Haematology (BCSH) for the Diagnosis and classification of acute leukemia are as follows: T-Lymphoid markers: CD3 (cytoplasmic) CD2 CD7 Myeloid markers: CD13 CD117 anti-MPO (cytoplasmic) CD33 CD41 CD42 CD61 anti-Glycophorin A B-Lymphoid markers: CD19 CD22 (cytoplasmic) CD79a (cytoplasmic) CD10 Cytoplasmic µ Surface membrane Ig CD138 Non-lineage restricted: TdT CD45 HLA-DR
Immunological subtypes of Acute Leukemia • ►B-ALL (B-lineage markers are positive), ≈75% of ALL • pro B-ALL • common ALL (CD19+/CD10+/TdT+/CD34+/-)…THE MOST COMMON • B-ALL (the most mature) (CD34-ve/cytoplasmic and surface Ig positive) • ►T-ALL (T-lineage markers are positive), ≈15% of ALL • ►AML (Myeloid lineage markers (CD13/CD33, CD117, cyMPO) are positive • ►Bi-lineage • ►Bi-Phenotypic
Cytogenetics/molecular genetics findings in ALL (as example) ONLY FOR YOUR REVIEW
ALL-L1 Small and homogenous blasts. These may closely resemble lymphocytes but are distinguished by their finer chromatin structure and the occasional presence of nucleoli
ALL-L2 Lymphoblasts of varying size (small and large)
Large blast cells with marked cytoplasmic budding (blebing). The differential diagnosis will be: AML-M7 and ALL. Farther cytochemical and immunophenotyping studies showed to be case of B-lineage ALL.
Auer rods in AML (pathogmonomic for myeloid lineage origin), A case of AML-M3