Download
1 / 44
450 likes | 693 Views
The Leukemias. Sherron R. Helms, M.D. March 24, 2005. Leukemias. Proliferation of abnormal clone of hematopoietic cells Poor response to normal regulatory signals Diminished capacity for differentiation Ability to expand at expense of normal cells Ability to suppress growth of normal cells.

E N D
The Leukemias • Sherron R. Helms, M.D. • March 24, 2005
Leukemias • Proliferation of abnormal clone of hematopoietic cells • Poor response to normal regulatory signals • Diminished capacity for differentiation • Ability to expand at expense of normal cells • Ability to suppress growth of normal cells
Leukemias- Etiology • Generally unknown • Host susceptibility- DNA repair mechanisms, Down syndrome • Chromosomal damage- physical (XRT) or chemical (alkylating agents, benzene) • Viral- EBV in Burkitt, HTLV-I in T cell ALL
Leukemias- Diagnosis • Generally requires bone marrow biopsy and aspirates with flow cytometry and cytogenetics • CLL can be reliably diagnosed by flow cytometry on peripheral blood • There must be > 20% blasts in marrow for diagnosis of acute leukemia
Leukemias- Classification • Acute vs Chronic • Based on natural history of the untreated disease • Myeloid vs Lymphoid • Based on the primary cell line involved
Leukemias • Lymphoid • CLL • ALL • Myeloid • CML • AML
CLL • Relatively indolent clonal lymphoid disease • Primarily B cell • Includes Hairy Cell Leukemia • Most common leukemia in adults • Median age at diagnosis: 62 y • Etiology unknown • Morphology: Normal B cells
CLL- Molecular Biology • Normal appearance, abnormal function • CD 5 expression • Defective apoptosis • Overexpression of bcl-2 gene
CLL- Clinical Presentation • Asymptomatic • Lymphocytosis noted on routine CBC • Lymphadenopathy and/or splenomegaly in ~50% at diagnosis • Staph, Strep, Herpes infections common • Autoimmune hemolytic anemia in 10% • ITP in 2%
CLL- Immune dysfunction • CLL B cells produce reduced levels of immunoglobulin in response to antigenic stimuli • Quantitative and qualitative abnormalities in B, T, NK cells • Impaired complement activation
CLL- Staging • LOW RISK • Lymphocytosis only • Average survival >10 yrs • INTERMEDIATE RISK • + Adenopathy and/or splenomegaly • Average survival 7 yrs • HIGH RISK • + Anemia and/or thrombocytopenia • Average survival 1.5 yrs
CLL- Clinical course • Generally, indolent with gradual increase in lymphocytosis, adenopathy, splenomegaly. May be years before Rx required • Richter syndrome- ~5% transform to aggressive large cell lymphoma/leukemia • Develop fever, weight loss, worsening anemia & thrombocytopenia, rising lymphocyte count • Short survival, poor response to therapy
CLL- Treatment • No survival advantage to therapy at time of diagnosis in low risk patients • Indications for therapy: • B symptoms • AIHA, ITP (steroids) • Massive hepatosplenomegaly • Bulky adenopathy • Recurrent infections
CLL- Treatment Options-I • Chlorambucil- Oral alkylator, ~50% RR, rare complete response • Fludarabine- IV purine analog, 70% RR, 30% CR, prolonged T cell suppression • IVIG: Only in pts with repeated bacterial infections
CLL- Treatment Options-II • Monoclonal Antibodies • Rituximab- antiCD20; when combined with chemo, 95% RR, 68% CR • Alemtuzumab- antiCD52- effective in clearing blood and marrow; less effective on nodes. Prolonged, severe T cell suppression • Bone Marrow Transplantation- autologous and allogeneic under study for healthy pts under 70yo
Hairy Cell Leukemia • Male predominance • Cytopenias, splenomegaly • Therapy: Cladribine- nucleoside analog • Single course of therapy • 90% response rate • Responses very durable • Resistant disease- BL-22: MoAb antiCD22 + pseudomonas exotoxin induces apoptosis- 75% RR in clinical trials
Acute lymphoblastic leukemia • Malignant disease of early B and T cells • Aberrant differentiation and proliferation • Cells accumulate in marrow and suppress normal hematopoiesis • In addition to marrow and peripheral blood, involves nodes, liver, spleen, CNS, and skin
A.L.L. • 20% of adult leukemia • Most common malignant disease in childhood • Symptoms: fatigue, fevers, bone pain, infection, bleeding, adenopathy • CNS involvement in 5-10% • Blasts in peripheral blood in 90% • Leukostasis uncommon even with WBC 100,000
A.L.L. Treatment • Induction, consolidation, maintenance • Use multiple chemotherapy agents to prevent resistance (vincristine, prednisone, daunorubicin, asparaginase) • Use prophylactic Rx of CNS (intrathecal methotrexate and AraC) • Postremission chemo to eliminate minimal residual disease • Adults: 65-90% remission; 20-30% cure • Allogeneic transplants in high risk pts
A.M.L. • Most common acute leukemia in adults • Median age at diagnosis: 60 yrs • The most common type of leukemia induced by alkylating agents (nitrogen mustard [7y]) or epipodophyllins (VP16, 1-2 y)
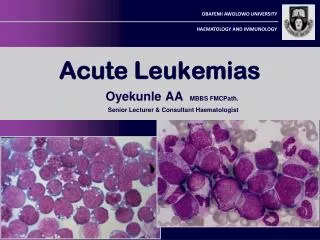
AML • Auer rods: accumulation of lysosomal granules in cytoplasm, seen in ~10% • Diagnosis by flow cytometry, cytogenetics on marrow • FAB classification has 8 subtypes (M0- M7); WHO classification has 19
AML- Clinical Features • Presenting symptoms: fatigue, bruising, infection • Acute promyelocytic subtype presents with bleeding, sometimes frank DIC • Acute myelomonocytic subtype often has gum and/or skin involvement • Leukostasis (pulm and CNS) common when blast count >50,000
A.M.L.- Therapy • Remission induction with cytarabine and daunorubicin • all-trans retinoic acid (ATRA) is added in acute promyelocytic leukemia (APL) • Postremission: consolidation chemo using high dose cytarabine for 2 cycles • 40% cure rate in young and middle aged adults • Maintenance therapy only in APL (ATRA) • Allogeneic transplant in high risk pts <70y who have match and are in CR
AML in Elderly • Poorer outcome, ~10% long term survivors • Less able to withstand intensive chemotherapy and complication of prolonged marrow suppression • Less marrow regenerative capacity • More often have poor-prognosis subtypes of leukemia • More often have MDS evolving into AML, multiple mutations and drug resistant
Acute Promyelocytic Leukemia (APL) • M3 subtype of AML • Promyelocytes contain granules with procoagulant and fibrinolytic activity • t(15;17) juxtaposes the RARa gene on 17 with the PML gene on 15 • The resulting PML/RARa represses transcription of the RAR needed for differentiation/apoptosis • High doses of ATRA cause release of the corepressor
A.P.L. • Retinoic acid + standard chemotherapy with daunorubicin and cytosine arabinoside (AraC) • 95% remission rate, 70% cure rate • Arsenic trioxide active in relapsed disease (causes histone acetylation, differentiation, & apoptosis)
Chronic Myelogenous Leukemia • A myeloproliferative disorder (CML, P. Vera, E.T.) • Clonal disorder of pluripotential stem cell • Median age 45-55 yrs • Philadelphia chromosome [t(9;22)] in 95%
CML • Expansion of myeloid cells at various stages of maturation • Three clinical phases: chronic, accelerated, and blast crisis • Patients proceed through these phases over ~4yrs if untreated • Symptoms: fatigue, night sweats, sx related to splenomegaly • High WBC, increased basophils, high platelet count
Ph Chromosome • BCR-ABL –protein product of the translocation • Transfection of BCR-ABL in mice causes CML • Inhibition of BCR-ABL in patients reverses CML • Acquired disorder • Cause of mutation unknown- radiation in some
Ph Chromosome- BCR-ABL • Tyrosine kinase activity • Leads to increased transcription of genes that control cell proliferation • Inhibits expression of cell adhesion molecules • Suppresses apoptosis
CML- Treatment • The BCR-ABL proteins must be phosphorylated to have tyrosine kinase activity • Imatinib (Gleevec) blocks phosphorylation • Oral agent, well tolerated • 87% RR, 76% complete cytogenetic response • Allogeneic stem cell transplant cures 75% of pts under age 70