Download

1 / 45
530 likes | 1.08k Views
Differential Diagnosis of Acute Abdominal Pain. SOAR-RN. Presented by: Jessicia Emory RN, MEd, CMSRN, CBN. The abdomen has many organs and complex structures. Determining the cause of abdominal pain is challenging even for experienced professionals. Introduction.

E N D
Differential Diagnosis of Acute Abdominal Pain SOAR-RN Presented by: Jessicia Emory RN, MEd, CMSRN, CBN
The abdomen has many organs and complex structures. Determining the cause of abdominal pain is challenging even for experienced professionals. Introduction TIP: Do not spend a lot of time trying to figure out the cause. Your goal in assessing abdominal pain is to determine if the patient is SICK or NOT SICK, and initiate care.
Esophagitis GERD Gastric ulcer Gastritis Duodenal ulcer Duodenitis Gastric outlet obstruction Bowel obstruction Intussusception Bowel perforation Cancer Hepatitis Splenic infarct Splenic abscess Mesenteric ischemia IBS Crohns disease Ulcerative colitis Gastroenteritis Appendicitis AAA rupture Esophageal spasm Diverticulitis Endometriosis Vitamin D deficiency Adrenal insufficiency Pancreatitis Cholangitis Cholecystitis Choledocholithiasis Incarcerated hernia UTI Nephrolithiasis Uterine pathology HIV Hemophilia Sickle cell disease Trauma Pneumonia Subdiaphragmatic abscess Myocardial infarction Pericarditis Prostatitis Idiopathic inflammatory disorders Abdominal wall pain Ectopic Pregnancy Just A Few Diagnoses to ponder….
Lets review: Anatomy Types of pain Assessment How Do You Decide Sick Or Not Sick?
The abdomen is the largest cavity in the body. The diaphragm separates the abdominal cavity from the chest cavity. Most of the abdominal organs are enclosed within the peritoneum. Those organs behind and outside the peritoneum include the kidneys, pancreas, and abdominal aorta. Anatomy
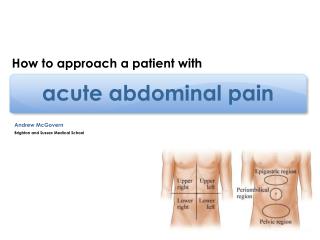
Four Quadrants Right upper quadrant (RUQ) contains the liver, gallbladder and part of the large intestine. Left upper quadrant (LUQ) contains the stomach, spleen, pancreas and part of the large intestine. Right lower quadrant (RLQ) contains the appendix, small intestine, fallopian tube and ovary. Left lower quadrant (LLQ) contains the small and large intestine, fallopian tube and ovary
Caused by stimulation of nerve fibers within internal organs or the tissues that support them. Poorly localized Hollow Organ Described as crampy, colicky, dull and intermittent. Solid Organ Described as pressure-like, deep, stabbing, dull and constant. Often associated with nausea, vomiting, tachycardia, and sweats. Types Of Pain Visceral Pain
Focal pain that occurs when never fibers within the peritoneum are irritated by chemical or bacterial inflammation. Localized pain Usually unilateral Described as sharp, knife like, distinct, and constant Causes tenderness and guarding which progresses to rigidity and rebound as peritonitis develops Made worse with coughing or movement Types Of Pain, Continued.. Parietal (Somatic) Pain
Visceral pain that is felt away from the actual affected organ site. Produces symptoms not signs Based on nerve pathways developed during embryonic development. Ureteral obstruction → bilateral flank pain, testicular pain Subdiaphragmatic irritation → ipsilateral shoulder or supraclavicular pain Gynecologic pathology → back or proximal lower extremity Biliary disease → right infrascapular pain MI → epigastric, neck, jaw or upper extremity pain Types Of Pain, Continued.. ReferredPain
Abdominal pain can be caused by: Blockage of a duct Swelling of a body structure Inflammation or stretching of an organ Loss of blood supply (ischemia) to an organ Causes of Pain
Pain location drives evaluation Pain Location
Cholecystitis Inflammation of the gallbladder caused by duct obstruction with a gallstone Pain is usually steady for an hour or more after onset and made worse by eating If there is significant inflammation there may be local peritoneal pain (somatic pain) Pain may be referred to the scapular area and accompanies nausea, vomiting, and fever without jaundice. RUQ Pain
Cholangitis Obstruction of the biliary tract leading to bacterial overgrowth in the gall bladder. Marked by Charcot’s Triad- RUQ pain, jaundice, and fever Diagnosed with ultrasound Emergent and must be treated with IV antibiotics May require decompression via endoscopic or surgical procedures. RUQ Pain
Hepatitis Caused by inflammation of the liver by viruses, alcohol, or certain drugs. Tender, enlarged liver with malaise, fever, and jaundice. Diagnosed by history and laboratory evaluation (liver function tests and viral serology) Treatment depends on etiology of disease. RUQ Pain
Pancreatitis Most commonly caused by alcoholism (50%) and gall stones (30%) obstructing the common bile duct. Constant mid-epigastric visceral pain usually occurring after a heavy meal or alcoholic binge. Pain may radiate to back (50%) and is accompanied by nausea, vomiting, and anorexia. Diagnosed by amylase and lipase. Imaging by CT scan in some cases RUQ Pain
Peptic Ulcer Disease Caused by increased gastric secretion (alcoholism or gastrin producing tumor) or decreased mucosal protection (overuse of NSAIDS or H. pylori infection) Pain is visceral but may become somatic if perforation occurs. There may be radiation to the back. Diagnosed by H.Pylori serology, abdominal x-rays, UGI, and endoscopy. LUQ Pain
Dissecting Abdominal Aortic Aneurysm Caused by tearing of the layers of the abdominal aorta secondary to atherosclerotic changes. Pain is an excruciating tearing sensation often referred to the midline back. May be accompanied by hypotension, pulsatile abdominal mass and diaphoresis. Diagnosed by abdominal ultrasound Is a surgical emergency LUQ Pain
Diverticulitis Diverticula form in weakened areas of the colonic wall and may become impacted with feces leading to infection and perforation. Crampy, steady visceral pain. May be accompanied by a change in bowel function, fever, nausea, vomiting, and anorexia. Diagnosed by CT scan Must avoid colonoscopy and barium enema in the acute setting to avoid perforation LLQ Pain
Ovarian Cysts Pain caused by distention of cyst lining which may hemorrhage into the pelvic cavity. Constant, achy pain in the lower quadrants which may radiate to the groin area. Diagnosed by ultrasound. Also consider ovarian torsion, pelvic inflammatory disease, and ectopic pregnancy. LLQ Pain
Appendicitis Caused by obstruction of the appendiceal lumen usually by a fecalith Pain starts as periumbilical and migrates to the RLQ (McBurney’s Point). Is accompanied by nausea, vomiting, and anorexia. May have fever-especially if ruptured. Diagnosed by CT scan. Emergent if ruptured RLQ Pain
Crohns Ongoing disorder that causes inflammation of the GI tract Pain is usually located in the RLQ Is accompanied by diarrhea, weight loss, a low grade fever, anemia, and sometimes constipation R/T a blockage Diagnosed by upper and lower GI. RLQ Pain
Some causes of abdominal pain are generalized and not restricted to any specific quadrant General Abdominal Pain
Ulcerative Colitis Inflammatory bowel disease (IBD) that affects the large intestine (colon) and rectum. Diffuse abdominal pain that usually disappears after a bowel movement. Is accompanied by bloody diarrhea, pus or mucus in the stool, and frequent fever. Diagnosed by colonoscopy. General Abdominal Pain
Gastritis Caused by inflammation of the gastrointestinal tract by microorganisms, radiation, and other irritants. Diffuse, crampy pain. Often accompanied by diarrhea, nausea, vomiting, dehydration, and fever. Diagnosis is by history and stool cultures if indicated. General Abdominal Pain
Colon Cancer Neoplastic growth in the ascending, transverse, descending, or sigmoid colon. Colicky pain. Associated with change in bowel habits, heme positive stools, and weight loss. Diagnosed by rectal exam, colonoscopy, flexible sigmoidoscopy and barium enema General Abdominal Pain
Determine if the patient is SICK or NOT SICK and initiate care. Assessment Goal
“OLD CARS” O- onset L- location D- duration C- character A-alleviating/aggravating factors R- radiation S- severity Assess key systems: Vital signs Respirations Mental Status Body position Abdominal assessment Look, listen, and feel Cardiac status Skin integrity Urine output Initial Assessment Tip: In the face of vague or confusing signs and symptoms, determine SICK or NOT SICK, and initiate appropriate care.
An alert and oriented 32 year-old male who is complaining of severe RLQ pain 10/10. He describes the pain as “sharp like someone is stabbing me”. He is guarding his abdomen and won’t let you touch it. Temp-38.8, RR-26, HR-120 with a thready pulse, BP 82/40. 60ml urine output for the last 4 hours The patient is nauseated and vomiting. He is pale and diaphoretic Case Study #: 1 SICK or NOT SICK?
Can you guess at a diagnosis? What makes you think he is sick? What are you going to do about it? SICK
ABC’s Initiate RRT Call MD Anticipate: CBC Chemistry Abdominal CT Fluid bolus Surgical intervention NPO Medicate for pain/nausea Interventions
41 year-old female complaining of LLQ pain rated a 5/10. She has a history of nausea and vomiting for the last 24 hours. Temp-36.8, Resp-16, HR-72, BP-122/60 She is alert and oriented and resting quietly in bed. Her skin is warm and dry. Case Study #2 SICK or NOT SICK?
Can you guess at a diagnosis? Why don’t you think she is sick? What are you going to do about it? NOT SICK
Medicate for pain/nausea Reposition Heat or cold therapy Alternative pain methods Interventions
A 22 year-old female with severe 8/10 LLQ and back pain Temp-37.4, Resp-24, HR-118, BP-80/46 The patient had an episode of syncope, but is now alert and oriented. She does c/o dizziness with movement. Her skin is pale, cool, and dry. She states that she is possibly pregnant. There is a small amount of vaginal bleeding present. Case Study #3 SICK or NOT SICK?
Can you guess at a diagnosis? Why do you think she is sick? What are you going to do about it? Sick
ABC’s Initiate RRT Call MD Anticipate CBC Chemistry Beta HcG Possible ultrasound Fluid bolus Surgical intervention NPO Medicate for pain/nausea Keep pt. on bedrest Interventions
A 56 year old male who is one day S/P gastric bypass. He complains of diffuse abdominal pain 8/10 radiating to his left shoulder. Temp-39.0, HR-sustained in the 130’s, RR-32 and shallow, BP-90/54, UOP <120ml/4 hours. He is slightly disoriented to place and time. His JP drain is putting out bile green fluid Case Study #4 SICK or NOT SICK?
Can you guess at a diagnosis? Why do you think he is sick? What are you going to do about it? Sick
ABC’s Initiate RRT Call MD Anticipate: CBC Chemistry Abdominal CT/CXR Fluid bolus Surgical intervention NPO Transfer to the ICU Medicate for pain/nausea Interventions
A 46 year old male who presents to the unit with profuse, watery diarrhea with frank blood and mucus which started “about four days ago.” He complains of diffuse abdominal pain rated 9/10. The patient also states that he has had a 20 pound weight loss, due to the inability to eat related to nausea. Temp-39.2, HR-98, Resp-18, BP-122/62 His hemoglobin and hematocrit are 11.2/36.1. (Normal hemoglobin 13.9-16.3, hematocrit 39-55) Case Study #5 SICK or NOT SICK?
Can you guess at a diagnosis? Why do you think he is sick or not sick? What are you going to do about it? Sick or Not Sick?
ABC’s Medicate for pain/nausea Fluid volume replacement Labs: Serial H/H Stool cultures to R/O infectious gastritis Endoscopy (upper and lower) Interventions
Although abdominal pain can be tricky to diagnose and treat, remembering which structures lie in which body section and understanding the different types of pain can help you gather the clues necessary to determine if your patient is sick or not sick. Conclusion