Download
1 / 20
200 likes | 423 Views
Computer aided diagnosis application in digital mammography and acute abdominal pain. By. Dr . Usama Gameel Bassuoni Executive manger of HMIS. Director of medical training Ahmed Maher Teaching Hospital. Medical decision process 3 element’s . · Information gathering · Data analysis

E N D
Computer aided diagnosis application in digital mammography and acute abdominal pain By Dr . Usama Gameel Bassuoni Executive manger of HMIS Director of medical training Ahmed Maher Teaching Hospital
Medical decision process 3 element’s ·Information gathering ·Data analysis ·Decision making ·“Human life is too important to be left to a computer“ Patients receive the best treatment on the best evidence available
· We must accept our limitations · Computers allow us to access up to date research worldwide · research is there to assist us not undermine our ability Shared information advances our knowledge . Encourages us to expand our practices . Scrutiny of all research to validate validity . No one person can have all expert knowledge it is important to collaborate with all professional colleagues ·Use good karma always
·is a soft ware ·is an increasingly role as decision making tool’s ·are being applied in several health care areas e.g digital mammography and AAP CAD CAD CAD
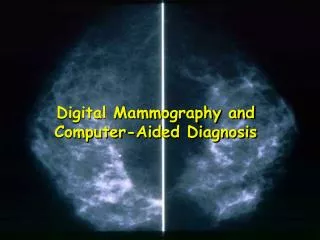
CAD in digital mammography ·Cancer Breast ♂ : ♀ 1-15 ·40% of CA Breast Benign · In Norway 2100 new cases,800 deaths/year ·Early detection↓mortality · Screening program based on mammography↓mortality · ↑no of countries started mass screening programs→increasedno mammography interpretation.
·Abnormalities embedded , camouflaged by varying densities of breast tissue · 10 – 30 % of ca breast missed by radiologist ·CAD design to detect , classification clustered micro calcification nodules
·Image segmentation : detection , extraction of clustered micro calcified nodules from back ground breast tissue ·Extracted micro calcification nodules categorized as benign or malignant ( image classification )
·Clustered micro calcification early signs ( potential cancerous changes) · Micro calcification small ca ++ deposit accumulate is breast tissue as a bright spot ·Cluster defined to be at least 3 micro calcifications with in 1-2 cm region of mammogram ·Individual micro calcifications range 0.1 – 1.0 mm ( in mammogram)
·Main goal of ACD system provide a second opinion ·2nd opinion radiologist use result of pc analysis of mammogram in making a diagnosis ·Digital mammogram → feature extraction → classification → analysis → detected tumor.
The main goal of CAD is to develop feature extraction schemes : ·To generate segment the mammogram into 2classes clusters of micro calcification normal tissues ·To generate features used to discrimination benign and malignant clusters of micro calcifications
CAD support in AAP Over last 20 Years studies in U.K , Europe in AAP shows : · 2-3.000.000 / year with AAP ·Cost Euro 1.5 million/ year ·AAP not a diagnosis in the strict sense but rather a symptom
·The most common frequent decision which surgeon called upon is not merely related to precise diagnosis but rather to operate or observe? · General rules of investigation : Know what you are doing? don’t waste time?, know what you want ?
·Main goal early diagnosis and correct management · Initial diagnosis accuracy 45 % ·Perforated app rate 30% (delayed diagnosis ) , -ve app rate 30% ·In Europe last year 200.000 app removed too late , 200.000 normal app removed
Health care data classified into 4 categories : . Patient centric data ( direct related to patient ) .Aggregates data based on performance and utilization ( resources management data) .Transforming – based data for planning , clinical and management decision support .Comparativedata for health services researches.
Computer aided decision support system “ CADSS “ • is AAP began in 1970 by professor Tim de-Dambal • Decision making improved by fall in –ve laprotomy and • rate of perforated appendicectomies
Initial diagnostic accuracy rate rose from • 45.6% - 63.5 % • -ve laprotomy rate fall by almost half • perforation rate amongst patient with appendicitis • fall 23.7 % - 11.5 % • Mortality rate fall by 22.0% • Direct cost saving of over 5 m Euro
CAD useful system for improving diagnosis and better clinical practice • 450 physician is 64 hospitals is 19 countries • ↓ residual diagnosis error rate by 40% • ↓ unnecessary operation by 25% • ↓ in perforation rate of appendicitis case by half
Changes is like dragon fight it you will loose .,ignore it., it will eat you., success only favors those who challenge it. Patients needs change constantly so therefore we must respond accordingly to new advancement in technology