Download
1 / 86
860 likes | 1.05k Views
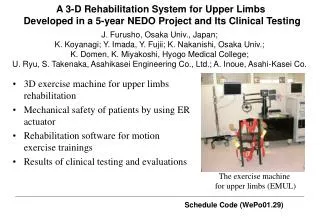
EXERCISE FOR OPTIMIZATION OF WORK PERFORMANCE AND OCCUPATIONAL REHABILITATION. WORK DEMANDS. Physical Task Demands. Work Content. Mental Task Demands. Required Qualification Processor. Physical Environment Demands. Work Context. Non-physical Environment Demands.

E N D
EXERCISE FOR OPTIMIZATION OF WORK PERFORMANCE AND OCCUPATIONAL REHABILITATION
WORK DEMANDS Physical Task Demands Work Content Mental Task Demands Required Qualification Processor Physical Environment Demands Work Context Non-physical Environment Demands
Job placement assessment Job Modification Education & Training Work Conditioning Work Demands Workers’ Qualification
Seating Standing Walking Kneeling Squatting One-legged Crouching Crawling Climbing Others Extremity postural Demands
Repetitive work Body segment Force and Posture Static work
Seating Standing Walking Kneeling Squatting One-legged Crouching Crawling Climbing Others Dynamic work Extremity postural Demands Static
Aerobic Energy System Anaerobic Circulatory Function Cardiorespiratory System Heart Function Respiratory Function ROM Physical Fitness Flexibility Joint Tissue Muscular Neuromuscular System Neural Fat Mass Body Composition Fat-free Mass
Biomechanical Physiological Psychological Stress Strain Disorders
TISSUE RESPONSES TO PHYSICAL STRESSORS Load Response Symptoms Adaptation Impairment Disability
TYPICAL PHYSICAL WORK DEMANDS OF TEACHER • Standing
WORK RISK FACTORS OF PROLONGED STANDING • Circulation • Muscle fatigue • Joint compression
Develop and improve: • Strength • Endurance • Cardiovascular fitness • Mobility • Flexibility • Stability • Co-ordination, balance and functional skills Work Demands
Introduction • Low back pain is the most common work-related msuculoskeletal disorders, and cause most socio-economical burden. • LBP claims account for 16% of all workers compensation claims and 33% of total claims costs (Bernard et al., 1997)
Definition • Prevalence • percentage of people in a certain population who suffer from the condition concerned • Point Prevalence • percentage who are found to be suffering at a certain moment in time ( i.e. when the survey is conducted)
LBP Prevalence • About 70% of people will suffer from one or more episodes of LBP at some time or another during their lives Bernard 1997
PREVALENCE OF LOW BACK DISORDERS • Local: • 39% in general population (Lau et al., 1995) • 58% in a group of manual handling workers
LBP Natural History • Most episodes of LBP are relatively short-lived (subsided within 6 weeks). • Recurrent rate is very high (60%) Biering-Sroenson 1983
Sickness Absence • 6 months absence: likelihood of returning to work fall to about 50% • After 1 year absence: 25% • After 2 years absence: virtually nil
Work-Related Risk Factors • Physical Factors • Heavy physical work • Lifting and forceful movements • Bending and twisting • Whole body vibration • Static work postures • Non-physical factors • Psychosocial factors Bernard 1997
EFFECTS OF PHYSICAL ACTIVITIES IN THE PREVENTION OF LBP • Strong evidence that PA has a primary preventive effect on LBP
EFFECTS OF PA IN SECONDARY PREVENTION (Van Tulder et al., 2000) • Acute LBP - strong evidence that exercise therapy is NOT more effective than inactive treatments or other active treatments. • Low stress aerobic activity during the first 2 weeks is indicative to improve recovery and lessen disability.
Chronic LBP – strong evidence that exercise therapy and conventional physiotherapy are equally effective and exercise therapy is more effective than usual care by GP • Strong evidence that strengthening exercises are more effective than other types of exercise. • Strong evidence that exercise diminishes the musculoskeletal and cardiorespiratory effects
TYPES OF EXERCISE AND TRAINING PRINCIPLES • FITT • TYPES: STRENGTHENING • STABILIZER • ENDURANCE • STRENGTH • TYPES: MOBILIZING
RATIONALE: • Relationship between the probability of injury and percentage of strength capacity used by the worker at work. (Chaffin 1973) • Relationship between the incidence of firefighter back injuries and level of physical fitness. 7.1% least fit, 3.2% moderate, 0.8% most fit (Candy et al., 1979)
EFFECTS OF A FOUR-WEEK MUSCLE STRENGTHENING PROGRAM ON MAXIMUM ACCEPTABLE LIFTING LOAD Yeung SS. et al., 1998
METHOD • Subjects= university students (N=19) • Isokinetic measurements of back extensors, knee extensors, shoulder abductors, and elb. Flexors. • Maximal acceptable lifting load (psychophysical approach)
TRAINING PROTOCOL • 4 WEEKS OF TRAINING • LOAD: 80% PEAK TORQUE • WEEKLY ADJUSTMENT BY 5%
RESULTS • Significant training effect on MALL and back extensors
EFFECTS OF SQUAT LIFT TRAINING AND FREE WEIGHT MUSCLE TRAINING ON MAXIMUM LIFTING LOAD AND ISOKINETIC PEAK TORQUE OF YOUNG ADULTSWITHOUT IMPAIRMENTS Yeung SS., & Ng GYF 2000
METHOD • 36 University Students • Training approach: 1. free weight muscle strengthening program; 2. Task specific training programme; and 3. Control
RESULTS • Significant improvement in MALL and back extensors • No significant differences between the training protocol
LOW BACK EXERCISES FOR LOW BACK DISORDERS McGill 1998
OBJECTIVES • To stress both damaged tissue and healthy tissues for tissue repair but avoid excessive loading • Exercises that challenge muscle but impose minimal joint loads
EXERCISE PRINCIPLES • Frequency: most beneficial when performed daily • No pain No gain ? • General conditioning exercise is important • Endurance more protective value than strength • Flexibility (mobilizing) should best be performed at unloaded position • No fixed recipes, exercise should be tailored made
BACK EXTENSOR EXERCISE • Pr lying arch back • ½ support back extension • Single leg extension with hand and knee support
ABDOMINAL EXERCISE • No single abdominal exercise challenges all of the abdominal musculature: • Curl-up challenges mainly RA • Sit-ups (leg straight or knee bent) = high psoas activation and disc compression • Leg raises causes even higher activation and compression • Isometric side support for QL
OCCUPATIONAL REHABILITATION • To facilitate a return to work or ensure an employee remains at work, ideally in his or her original job • Different terminology:work, industrial, vocational rehabilitation
Work Conditioning FCE Work Hardening Acute Mx Return to Work Work Demand Analysis Work Modification DISABILITY MANAGEMENT Injury
FUNCTIONAL CAPACITY EVALUATION • Functional: Meaningful, useful and purposeful • Capacity: maximum ability and capability • Evaluation: Systematic approach including observation, measurement, reasoning and conclusion
FUNCTIONAL CAPACITY EVALUATION • Systematic, comprehensive approach • Objective and valid measurements to predict a person’s ability to perform work related tasks.
FUNCTIONAL CAPACITY EVALUATION • Generic - Baseline Capacity Evaluation • Usually based on physical demands of DOT • Job oriented – Job capacity Evaluation • Focus on the match of the worker’s ability to the work demands of specific job • Worker oriented – Work capacity Evaluation • Determine worker’s capabilities to the basic demands of earning occupation
APPLICATION • Ensure workers’ health and safety in job placement (OSHA); • Identify an individual’s physical abilities and limitations (ADA) • Determine an injured worker wage-earning potential and return to work abilities (Insurance company and legal profession)
FCEs • ARCON • BLANKENSHIPS • TRACKER • BTE • ERIC • MVE Battery Tests • Non-computerized system
TYPICAL COMPONENTS OF FCES • Interview – patient information • Job analysis (questionnaire) • Behavioural profile • Physical measures/muscuoskeletal evaluation • Physiological measures • Functional measures • Comparison of testing with job requirements