Download
1 / 27
270 likes | 380 Views
FOR SASK RESPIRATORY SUMMIT ONLY DO NOT CIRCULATE. FOR SASK RESPIRATORY SUMMIT ONLY DO NOT CIRCULATE. Pauwels RA, et al. Lancet 2004; 364:616-620. Optimizing Chronic Disease Management. FOR SASK RESPIRATORY SUMMIT ONLY DO NOT CIRCULATE. Jamal A, et al. JAMA 2005; 294:1255-1259.

E N D
FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Pauwels RA, et al. Lancet 2004; 364:616-620
Optimizing Chronic Disease Management FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Jamal A, et al. JAMA 2005; 294:1255-1259
Optimizing Chronic Disease Management #4 #7 #12 FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE September 28th, 2006
Optimizing Chronic Disease Management SHR Hospitalizations FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Saskatoon Health Region Statistics, 2005
Optimizing Chronic Disease Management FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE SHR Hospitalizations Saskatoon Health Region Statistics, 2005
1.0 0.8 0.6 0.4 0.2 0 0 10 20 30 40 50 60 Optimizing Chronic Disease Management Exacerbations and Mortality Group A: no exacerbations Group B: 1–2 exacerbations Group C: ≥3 exacerbations A p<0.0002 Survival probability B p<0.0001 p=0.069 C FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE n=304 Time (months) Exacerbation = ER visit or hospital admission Soler-Cataluna JJ, et al. Thorax 2005;60:925–931
Myocardial Infarction 25% of men and 38% of women will die within 1 year of a first recognized MI (5,6) The in-hospital acute MI mortality rate is 9.4% (1999) (5,6) Optimizing Chronic Disease Management Acute Event Mortality FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE 1. Eriksen N, et al. Ugeskr Laeger 2003;165:3499–3502. 2. Groenewegen KH, et al. Chest 2003;124:459–467. 3. Almagro P, et al. Chest 2002;121:1441–1448. 4. Connors AF, et al. Am J Respir Crit Care Med 1996;154:959–967. 5. Thom T et al. Circulation 2006. 6. Heart and Stroke Foundation of Canada
COPD Exacerbation 22-43% of patients hospitalized with a COPD exacerbation will die within 1 year (1,2,3,4) The in-hospital mortality rate for COPD exacerbations is 7-11% (1,2) Myocardial Infarction 25% of men and 38% of women will die within 1 year of a first recognized MI (5,6) The in-hospital acute MI mortality rate is 9.4% (1999) (5,6) FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Optimizing Chronic Disease Management Acute Event Mortality 1. Eriksen N, et al. Ugeskr Laeger 2003;165:3499–3502. 2. Groenewegen KH, et al. Chest 2003;124:459–467. 3. Almagro P, et al. Chest 2002;121:1441–1448. 4. Connors AF, et al. Am J Respir Crit Care Med 1996;154:959–967. 5. Thom T et al. Circulation 2006. 6. Heart and Stroke Foundation of Canada
Optimizing Chronic Disease Management Risk of Death - Exercise Capacity FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Risk of death in subjects with risk factors and exercise capacity of <5 MET or 5-8 MET, compared with subjects with capacity >8 MET (MET = VO2 3.5 ml/kg/min) Myers J et al, NEJM2002; 346:793-801
FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Optimizing Chronic Disease Management Rehab and HealthCare Utilization Healthcare utilization over 18 months of follow-up. Data presented include physicians visits, telephone calls, hospital days, and urgent care visits over the preceding 3 months. The results are presented as mean + SE. Ries AL, et al. J Cardiopulm Rehabil 2004; 24(1): 52-62
Tiotropium Placebo Optimizing Chronic Disease Management Bronchodilators and Rehabilitation Study Drug * * Rehabilitation 32% 42% Endurance Time (mins) 16% * p<0.05 Weeks on Treatment FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Casaburi R, et al. Chest 2005; 127:809-817
Optimizing Chronic Disease Management Comprehensive COPD Management FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Bourbeau J, et al. Arch Int Med 2003, 163:585-91 *Can Respir J 2004; 11(Suppl B): 7B-59B
FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Optimizing Chronic Disease Management Comprehensive COPD Management • benefits persist over 2 years (Gadoury MA, et al. Eur Resp J 2005; 26:853-857) • a caseload of 50 patients equals cost-savings (program vs usual care) of $2,149 – $2,300 /year • concluded that a caseload of 70 patients was achievable and reasonable (additional savings of $310 /year) • reduced hospitalizations, reduced exacerbations, and reduced healthcare costs Bourbeau J, et al. Chest 2006; in press
Comprehensive CHF Management FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Ezekowitz, JA, et al. CMAJ 2005; 172:189-194
Preventing Type 2 Diabetes FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE n= 3234 non-diabetics with elevated fasting glucose Knowler WC, et al. NEJM 2002; 346:393-403
FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Optimizing Chronic Disease Management “Inspire” COPD Program • team-based, multidisciplinary program to help COPD pts and their families improve self-management of their disease • focused on outcomes • increased Pulmonary Rehabilitation capacity • home site (Field House) is full • assisted with establishing program in Regina • established 1st satellite in part of Saskatoon with the highest incidence of chronic diseases • additional satellites rolled out (Humboldt and Prince Albert) and other’s planned (Lawson Heights/Soccer, Saskatoon core, Yorkton, Moose Jaw)
FOR SASK RESPIRATORY SUMMIT ONLYDO NOT CIRCULATE Optimizing Chronic Disease Management What Have We Seen So Far? • reduced COPD re-admissions - net cost savings of ~129,000 in 2005, and ~$79,000 in 2006 • re-admission rates of 1 : 1.9 : 2.1 (2004), changed to 1 : 1.6 : 1.2 (2006) with recent programming at 3 acute-care sites in SHR • decreased ICU days by 44% (2006), with a cost savings in 2005 of $261,333, and in 2006 of $308,333. Saskatoon Health Region Statistics, 2006
Group Exercise and Rehabilitation • Community-based supervised exercise programming • Group education • Socialization
Group Exercise and Rehabilitation Patient Self-Management Skills • “Live-Well with a Chronic Condition” • Patient-led group classes / support • Enhanced self-management skills and decision-making • Community-based supervised exercise programming • Group education • Socialization
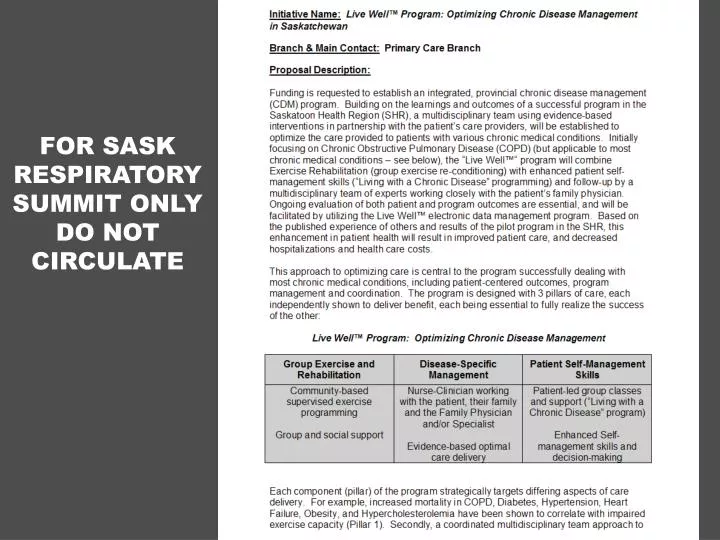
Group Exercise and Rehabilitation Disease-Specific Management Patient Self-Management Skills • “Live-Well with a Chronic Condition” • Patient-led group classes / support • Enhanced self-management skills and decision-making • Community-based supervised exercise programming • Group education • Socialization • Nurse-Clinician working with the patient, their Family Physician and/or Specialist • Evidence-based optimal care delivery
Live Well™ Program • a cost-effective, integrated [provincial] program - centralized coordination with both urban and rural delivery • strategic, focused design and delivery • “the right person doing the right job” • cement the relationship between the patient [and family] and their family physician • interventions that are not evidenced-based will not be utilized or promoted
Live Well™ Program (cont’d) • ongoing evaluation of both patient and program outcomes is necessary • an electronic data management system is used for patient care, and also to facilitate communication, coordination and evaluation • the program philosophy, design and delivery is common [ie. efficient] for many medical conditions – only Pillar 2 is “disease-specific” • the model works and borrows on the learning's of others
Live Well™ Program (cont’d) • proposed Centers of Excellence in Regina and Saskatoon, but with comprehensive program delivery in every health region, using an achievable phased implementation • benefits to patients are coupled with significant cost savings • targeted funding would best be provided “provincially” to the health regions with the expectation of tangible deliverables and appropriate evaluation/reporting