Download
1 / 45
460 likes | 635 Views
SUSAN VOSLOO CHRISTIAAN BARNARD MEMORIAL HOSPITAL CAPE TOWN. MODERN DAY APPROACH TO AORTIC COARCTATION. HISTORY. 1760 Morgagni Congenital narrowing of aorta adjacent to attachment of ductus Uncommon between LCA & LSA, or in lower thoracic or abdominal aorta. MORPHOLOGY.

E N D
SUSAN VOSLOO CHRISTIAAN BARNARD MEMORIAL HOSPITAL CAPE TOWN MODERN DAY APPROACH TO AORTIC COARCTATION
HISTORY • 1760 Morgagni • Congenital narrowing of aorta adjacent to attachment of ductus • Uncommon between LCA & LSA, or in lower thoracic or abdominal aorta AORTIC COARCTATION
MORPHOLOGY AORTIC COARCTATION
COARCTATION SEGMENT AORTIC COARCTATION
FETAL CIRCULATION AORTIC COARCTATION
CO-EXISTING LEFT HEART ANOMALIES (up to 50%) • Supravalvarmitral ring • Mitral stenosis with or without a single papillary muscle (parachute mitral valve) • Endomyocardial fibrosis • Left ventricular hypoplasia or hypertrophy • Aortic atresia and hypoplasia of ascending aorta • Supra-valvar, valvar, sub-valvaraortic stenosis or hypoplasia AORTIC COARCTATION
MAJOR COLLATERAL CHANNELS AORTIC COARCTATION
AGES AT PRESENTATION 1ST OPERATION (92) RECOARCTATION (8) (2.2%) 2 19 (20.6%) 40 (43.5%) 3 3 31 (33.7%) 2 AORTIC COARCTATION
AGES AT CLINICAL PRESENTATION • NEONATAL PERIOD (40) first month of life (12 pre-op vent, inotropes incl 5 isolated coarct, 7 co-existing lesions) • INFANCY (34) from 1 month - 1 year • CHILDHOOD (21) age 1 – 14 years • ADOLESCENTS AND ADULTS (5) beyond 14 years AORTIC COARCTATION
SPECIAL INVESTIGATIONS • ECHOCARDIOGRAPHY • CARDIAC CATHETERIZATION OR AORTOGRAPHY • MRI • CT AORTIC COARCTATION
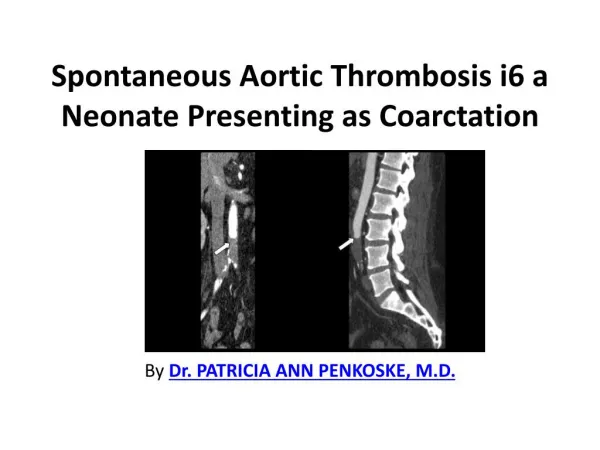
MR AORTIC COARCTATION AORTIC COARCTATION
CT AORTIC COARCTATION AORTIC COARCTATION
PRIMARY ANGIOPLASTY vs SURGERY OLDER PATIENTS: Primary angioplasty & stenting > surgery with comparable if not superior risk & recurrence rates HIGH RISK INFANTS: Still better served with surgery AORTIC COARCTATION
Do High-Risk Infants Have a Poorer Outcome From Primary Repair of Coarctation? Analysis of 192 Infants Over 20 yrs (JG McGuinness,et al, Our Lady’s Childrens Hospital, Dublin, Ireland, AnnThorac Surg 2010; 90:2023-2027) Primary angioplasty reports ( 8 studies last 10 yrs): • 6 studies represented only low risk pts, no initial mortality, re-intervention rate of 14-83% • 2 studies included high risk patients: • mortality 17 & 21% • re-intervention 73% in 10 days, 77% by 12 yrs • Both studies reported lost femoral pulses 12-18%, long term sequelae unknown AORTIC COARCTATION
Do High-Risk Infants Have a Poorer Outcome From Primary Repair of Coarctation? Analysis of 192 Infants Over 20 yrs (JG McGuinness,et al, Our Lady’s Childrens Hospital, Dublin, Ireland, AnnThorac Surg 2010; 90:2023-2027) Higher vs lower risk surgical pts (pre-op PG, ventilation, LV dysfunction, inotropic support) were: • Smaller (3.3 vs 4.2 kg), younger (18 vs 57 days), PAB (25 vs 15%), • same technique, similar X-clamp times • mortality(7 vs 3%), recurrence (11%) • treated easily with single balloon angioplasty,mean 3.8 yrs later AORTIC COARCTATION
SURGICAL HISTORY • 1944 Crafoord & Nylin • 1945 Gross • Original technique resection with end-to-end anastomosis (REE) • Other techniques followed • Choice of technique mostly based on individual preference AORTIC COARCTATION
SURGICAL APPROACH LEFT THORACOTOMY AORTIC COARCTATION
SURGICAL TECHNIQUES ALL OPERATIONS (n=100) 3 10 14 73 AORTIC COARCTATION
SURGICAL TECHNIQUES FIRST OPERATION (92) RECOARCTATION (8) 7 14 2 3 71 3 M/s (9) M/s (2) AORTIC COARCTATION
SIMPLE RESECTION & END-END ANASTOMOSIS (SEE) AORTIC COARCTATION
MONITORING PRE-REPAIR AORTIC COARCTATION
MONITORING POST-REPAIR AORTIC COARCTATION
EXTENDED RESECTION & END-END ANASTOMOSIS (Amato 1977) AORTIC COARCTATION
GROWTH & ARCH RE-INTERVENTION FACTORS • Mortality (8/36) and arch re-intervention (5/36) common in neonates weighing < 2.5 kgs • SEE (2/3); EEE (3/16); SCF (7/15); patch aortoplasty (1/2) • Catch-up growth of transverse arch and isthmus does occur post coarctation repair, especially in smallest arch parameters, where EEE was favoured • This may be increased using extended rather than simple resection and end-to-end anastomosis (T Karamlouet al: Hosp for Sick Children,Toronto; J ThoracCardiovascSurg 2009; 137: 1163-7) AORTIC COARCTATION
ALTERNATIVE SURGICAL TECHNIQUES • Subclavian flap & reversed subclavian flap • Patch aortoplasty (indirect aortoplasty) & Direct aortoplasty • Interposition or Bypass grafts AORTIC COARCTATION
SUBCLAVIAN FLAPWaldhausen & Nahrwold 1966 AORTIC COARCTATION
REVERSED SUBCLAVIAN FLAP AORTIC COARCTATION
DIRECT ISTHMOPLASTYVosschulte 1957 AORTIC COARCTATION
PATCH AORTOPLASTYIndirect Isthmoplasty AORTIC COARCTATION
CAUSES OF ANEURYSM • Accelerated proximal aortic wall growth due to compliance mismatch • Cystic medial necrosis in aortic wall adjacent to coarctation • Disruption of intima or sub-intima with or without patch aortoplasty • Infection AORTIC COARCTATION
ANEURYSMS POST COARCTATION REPAIR Predictors of aneurysm formation after surgical correction of aortic coarctation (Y von Kodolitsch, Hamburg, Germany, J Am Coll Cardiol, 2002; 39:617-624) Reported 25 aneurysms (9% of coarctation repairs),8 ascending, 17 local aneurysms, with 36% mortality if left untreated Independent predictors for aneurysm formation: * Higher age at repair (72% had surgery after age 13.5 yrs) * Patch graft technique * Higher pre-op gradient & bicuspid aortic valve favoured ascending aneurysm formation AORTIC COARCTATION
INTERPOSITION GRAFTS Schusler 1962 Brom 1965 AORTIC COARCTATION
BYPASS GRAFTSWeldon 1973 Edeie 1975 AORTIC COARCTATION
MID-TERM OUTCOMES OF RESECTION & EEE • 201 pts coarctation without/with VSD (14%) • Neonates (53%); pre-op shock(20%) • Sternotomy 44 pts (22%); thoracotomy 157 pts (78%) • Early mortality 2% (PHT&CDH, MAS, MOF, RSV) • Re-intervention 8 pts (3 balloon angioplasty; 5 re-ops; 75% in 1st po yr) (S Kaushal; Children’s Memorial Hosp, Chicago; Ann Thor Surg 2009; 88: 1932-8) AORTIC COARCTATION
OUTCOME - MORTALITY • No deaths < 1 month or > 1 year • 2 early deaths (both hospitalized since birth) 1. F, ex-prem, 6 weeks, 1.8 kg, pre-op vent, Coarctation & AP Window, po pneumonia, ECMO day 5-19, off ECMO, recurrent pneumonia week later, died respiratory failure 2. F, ex-prem, 3 months, 2.1 kg, large hydrocephalus, massive pericardial effusion, Klebsiellasepticaemia, died day 7 po • No late deaths, including all subsequent surgery for intracardiac repairs post palliation AORTIC COARCTATION
OUTCOME – EARLY MORBIDITY • Transient Hypertension common • PO Ventilation > 3 days (3 – 2 died) • Phrenic Nerve injury(2); Both required diaphragmatic plication • Chylothorax (2); 1 thoracic duct ligation • No postop bleeding, spinal cord complications AORTIC COARCTATION
FACTORS DETERMINING SPINAL CORD INJURY RISK • The location and length of narrowing • The presence of the collateral circulation • The clamping time required for the procedure AORTIC COARCTATION
OUTCOME – LATE MORBIDITY • PPM (2) – LV dysfunction at 1 & 4 yrs • Late Aneurysms – nil • Hypertension – continuous anti-HT therapy (2) • Recoarctation ( 8 single balloon angioplasty < 6m; 2 at 4 & 6 yrs po; 1 redo surgery REE – patch at 6m) AORTIC COARCTATION
CAUSES AORTIC RECOARCTATION AORTIC COARCTATION
PATIENTS (n=100) • ISOLATED COARCTATION (66) including 12 pts with stable left heart obstructive lesions, being observed • CO-EXISTING CARDIAC LESIONS (34) • M 58; F 42 • PRIMARY OPERATION (92) • RECOARCTATION (8) AORTIC COARCTATION
CO-EXISTING CARDIAC DEFECTS (n=46/100) • Bicuspid Aortic Valve (8) • Stable Shone complex (4) (12) • Significant LVOTO (5) (34) • VSD (16) • Other (13) DORV (4) TGA&VSD (2) UVH (5) AP-window (1) IHD (1) AORTIC COARCTATION
COARCTATION PLUS SIGNIFICANT LVOTO (n =5) • AORTIC VALVOTOMY (3) Aortic valvotomy with aortic coarctation (1), Aortic valvotomy at 3 & 5 months post coarct (2) • PROGRESSIVE LVOTO POST-COARCT REPAIR Ross procedure at 5 yrs (1) Resection Subaortic stenosis at 4 yrs,then Ross-Konno at 10 yrs (1) AORTIC COARCTATION
COARCTATION PLUS VSD(n = 16) • RECOARCTATION (4) Primary VSD & coarctation (2) PAB & coarctation; later VSD closure (2) • PRIMARY VSD & COARCTATION (3) • PAB & COARCTATION (9) CBMH; later VSD closure @ 4-22m age (5) RXH; all awaiting definitive procedures (4) AORTIC COARCTATION
COARCTATION WITH OTHER CARDIAC DEFECTS (n=13) • Primary repair with coarctation (5) - APW (1), - IHD (LIMA – LAD) (1); - TGA & VSD primary ASO & VSD (1), - DORV (2) • Palliation PAB (8) • TGA & VSD at 11m (1), • DORV at 11 & 15 m(2) • UVH: Glenn (3/5), TCPC (1/3) - Awaiting repairs(2) AORTIC COARCTATION