Download
1 / 1
10 likes | 158 Views
Case of the Week – 08-06: Coarctation & aortic stenosis. History: A 46 YO ♂ with 6 months breathlessness. Previous patch repair of “adult type” CoA. 12 lead ECG: LVH Echocardiogram: Bicuspid, calcified Ao valve, gradient 85mmHg. CMR referral: Evaluate status of CoA repair.

E N D
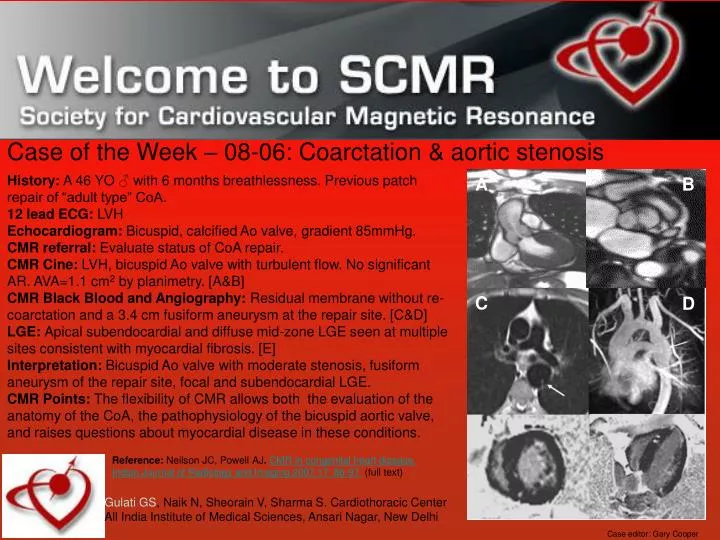
Case of the Week – 08-06: Coarctation & aortic stenosis History: A 46 YO ♂ with 6 months breathlessness. Previous patch repair of “adult type” CoA. 12 lead ECG: LVH Echocardiogram: Bicuspid, calcified Ao valve, gradient 85mmHg. CMR referral: Evaluate status of CoA repair. CMR Cine: LVH, bicuspid Ao valve with turbulent flow. No significant AR. AVA=1.1 cm2 by planimetry. [A&B] CMR Black Blood and Angiography: Residual membrane without re-coarctation and a 3.4 cm fusiform aneurysm at the repair site. [C&D] LGE: Apical subendocardial and diffuse mid-zone LGE seen at multiple sites consistent with myocardial fibrosis. [E] Interpretation: Bicuspid Ao valve with moderate stenosis, fusiform aneurysm of the repair site, focal and subendocardial LGE. CMR Points: The flexibility of CMR allows both the evaluation of the anatomy of the CoA, the pathophysiology of the bicuspid aortic valve, and raises questions about myocardial disease in these conditions. A B C D Reference: Neilson JC, Powell AJ. CMR in congenital heart disease. Indian Journal of Radiology and Imaging 2007;17: 86-97. (full text) Gulati GS, Naik N, Sheorain V, Sharma S. Cardiothoracic Center All India Institute of Medical Sciences, Ansari Nagar, New Delhi Case editor: Gary Cooper