Download
1 / 76
760 likes | 773 Views
This conference discusses various types of rashes in children, including bullous dermatosis, candidiasis, cellulitis, coccidioidomycosis, ecthyma gangrenosa, eczema herpeticum, foot ulcer, granuloma annulare, Henoch-Schoenlein purpura, impetigo, Job's syndrome, Kawasaki syndrome, leishmaniasis, lupus, meningococcemia, MRSA, nephrotic syndrome, neutropenia, osteomyelitis, peritonitis, Pott's puffy tumor, Q-taneous larva migrans, Ritter Disease, STDs, shingles, SJS, Sweet's, tinea, toxoplasmosis, TB, ulcerating hemangioma, varicella, warts, and more.

E N D
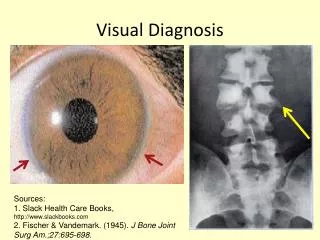
Visual Diagnosis:The ABCs of Rashes in KidsNoon ConferenceP.S.: It’s not all about HIV. Ann Petru, M.D. Pediatric Infectious Diseases October 23, 2009
Bullous dermatosis Candidiasis, Cellulitis Coccidioidomycosis Ecthyma gangrenosa Eczema herpeticum Foot ulcer Granuloma annulare Henoch-Schoenlein purpura Impetigo Job’s syndrome Kawasaki syndrome Leishmaniasis Lupus (Congenital, SLE) Meningococcemia, MRSA Nephrotic syndrome Neutropenia Osteomyelitis Peritonitis, Pott’s puffy tumor Q-taneous larva migrans Ritter Disease (SSSS) STDs, Shingles, SJS, Sweet’s Tinea,Toxoplasmosis, TB Ulcerating hemangioma Varicella Warts, Yuck (pus) Zebras……… and more. Alphabetical List of Topics
Behcet’s disease • 14 yo boy referred to ID clinic • 5 year hx of oral ulcers • Intermittent fevers • 6 wks of foot pain, redness, swelling • ESR 93, WBC 9.6 • Occasional bloody stools • Weight loss • Presented 6 months later with acute chest pain and ECG changes. • Eventually diagnosed with coronary aneurysm/fistula and subendocardial myocardial infarction with severe MV disease.
Bullous dermatosis • 13 yo Tongan has recurrence of this rash after 3 years in New Zealand • Rapid evolution • UCSF bx: Bullous pemphigoid or Linear IgA bullous dermatosis • B.P. is usually men 60-80 yo • Linear IgA dz - rare, autoimmune, linear deposits of IgA along basement membrane • Pruritic, annual papules, vesicles and bullae in groups; predilection for extensor surfaces, symmetric • Collarettes: blisters form as new lesions arise in periph. of old ones • Subepidermal PMN infiltrates • Rx: Dapsone and steroids
Candidiasis • 3 mo old boy with diaper rash: Candida albicans • Fussy, hard to console. Seems to ‘burn’ with every wet diaper • Characteristic ‘satellite’ lesions at edges • ‘id’ reaction - severe inflammatory component • Mgmt: Oral antifungal & topical steroids to control inflammatory reaction • Response was excellent
Cellulitis of the chest wall • 14 mo with rapidly progressing swelling • Seen in ER, T 102 • WBC 18K (72 polys, 12 bands) • ESR 48, CRP 6 • Blood culture sent • Needle aspirate: pus obtained --> GS: GPC • Most likely organism: Staphylococcus aureus • Big concern in 2005? MRSA * Empiric antibiotic choices? Clinda vs Vanco vs TMP-SMX +/- rifampin
Cellulitis of the neck, premie • Growing premature infant, was 2 weeks old and doing fairly well, breathing on his own, until… • He crashed: reintubated, cultured, antibiotics started • Blood: Group B Streptococcus • Rx amp/gent x 3 wks • Recovered fully • No meningitis! • Remember: GBS may recur (GI colonization)
Group B Strep cellulitis-adenitis syndrome • Abrupt onset of fever, poor feeding, and irritability • Unilateral non-discrete facial or submandibular swelling - erythematous and tender. • Bacteremia usually present, • GBS isolated from aspirate of cellulitis or LN • Ipsilateral otitis media is common. • Suppurative submandibular lymphadenitis caused by S. aureus is distinguished by manifestation as a discrete mass and propensity for suppuration.
Coccidioidomycosis • 12 year old boy from the Central Valley was referred to CHRCO for evaluation of this skin lesion • Local dermatologist had done a biopsy, which grew Coccidioides immitis ! • Cutaneous ‘cocci’ had not been seen in our clinic before • Treated with oral antifungal and had an excellent response
Coccidioidomycosis • Coccidioides immitis… dimorphic soil fungus. • Spores are airborne and lead to disease. • Primary infection: respiratory • 60% asymptomatic or self-limited • Sympt.: flu-like, fever, cough, malaise, • myalgia, headache and chest pain • Diffuse rash, EM, erythema nodosum, arthralgia • 5% may develop pulmonary scars • Extrapulmonary is rare, follows trauma, • soft tissue infection • Dissemination is rare (<1%) • Dx: Culture (warn lab; danger with aerosol- • ization of organism in lab); serology (UC Davis • c/o Dr. Pappagianis). • Rx: Ampho B (severe) or itraconazole • or fluconazole (oral)
Cutaneous coccidioidomycosis • Another teenager • Central Valley • Chronic skin problems • Biopsied by local MD, sent to us. • Cx: + for cocci • Rx: Underway with fluconazole
Ecthyma gangrenosa • 14 yo boy with acute myelogenous leukemia (AML) for past 2 years. Prior pneumonia (scar) was due to Rhizopus infection (bx); AML now relapsed and out of control • E.G. => Painful, widespread lesions • His culture from one grew Fusarium species • Gram stain usually positive in cases with EG • Other bugs: Pseudomonas, Vibrio species
Eczema = Atopic Dermatitiswith secondary infection • 11 yo with 2-3 week hx of itchy rash, started on right leg, spreading rapidly. Nontoxic. Some areas ooze purulent material. No prior dx of atopic dermatitis! • Cx: Meth-sensitive Staph aureus • Dry, itchy, scratched areas become darker & thickened (lichenified) • Predisposed to become infected • Commonly Staph aureus and Strep Gp A • Rx includes aggressive skin care with moisturizers, antihistamines, and potent antibiotics (IV for this).
Eczema herpeticum (HSV) 12 month old boy with severe eczema Thickened, rough skin despite creams Itching all the time Kissed by a loving relative with a cold sore - no thanks! Rx: IV acyclovir, antihistamines, skin care
Excessive prolif. of keratinocytes • Thickened, scaly plaques; itching • Inflammatory changes of epidermis and dermis. • Guttate psoriasis distinctive acute form in children and young adults • Closely associated with preceding sore throat, tonsillitis, Strep infxn Guttate Psoriasis
Henoch-Schoenlein Purpura Also called Anaphylactoid Purpura Is this rash an infection? 5 month old boy awoke with swollen hands, feet and face.
Henoch-Schoenlein Purpura • HSP is a vasculitis of small blood vessels • Cause is unknown, typically follows URI • Children > adults, males > females, 9/100,000. • Mostly 2-8 yo, winter months • Lab studies are nonspecific and not diagnostic • Acute onset sx, low-grade fever, fatigue, RASH • Main consequences: GI (colicky pain, blood in stools, diarrhea), kidneys, and arthritis (edema). • Prognosis good; steroids for GI dz only.
Job’s syndrome (Hyper IgE syndrome) • Rare disorder, autosomal dominant inheritance (var) • Mucocutaneous candidiasis (yeast) early in life • Recurrent infections (pneumonia, skin, eczema) • High IgE (>2000 IU/ml) • Eosinophilia • Dental problems • Scoliosis, fractures Common pathogens (lungs, skin, abscesses): Haemophilus influenzae, Strep pneumoniae, Staph aureus
Job’s syndrome: Eczema and secondary Staphylococcal infections
Leishmaniasis • 6 yo boy went to Middle East with family for 2 mos • 3 lesions developed on arms, leg, spreading. Biopsy done. • An older man asked, “Could this be an oriental sore?” • Google: “oriental sore” = Leishmaniasis. • It’s all in the history (and modern technology) • Bite of infected sandfly, inoculates parasites (Leishmania)
Leishmaniasis • 3 different clinical syndromes • Cutaneous:sandfly inoculates parasites into skin, proliferate in local phagocytes -> nodule, ulcer with raised borders, face & extremities in exposed areas, local lymph nodes react. Spontaneous resolution, weeks to years, flat scar • Mucocutaneous (espundia):from skin parasites disseminate to oral and nasopharyngeal mucosa, sometimes ulcerate, scars, mucosal perforation • Visceral (kala-azar):Skin through mononuclear macrophages, concentrated in spleen, liver, bone marrow -> fever, anorexia, weight loss, HSM, enlarged lymph nodes, anemia, low WBC, low platelets, low albumin, and high Igs. Untreated: fatal.
Congenital (Neonatal) Lupus Baby whose mother had SLE: • Due to placental transfer of IgG autoantibodies between 12-16th week of gestation to baby • Manifestations: congenital heart block, cutaneous lesions, liver disease, low platelets, low WBC, pulmonary and neurologic disease. • Most manifestations resolve but congenital heart block requires pacemaker. • This baby recovered gradually over a few months. Rash mimics serious infections, such as meningococcemia.
Systemic lupus erythematosus • SLE is a rheumatic disease of unknown cause • Autoantibodies directed against self-antigens Inflammatory damage to target organs • Kidneys, blood cells, central nervous system • Diff Dx: FUO, arthralgias, anemia, nephritis • Dx: autoantibodies: antibodies to DNA, ribosomes, platelets, coagulation factors, Ig’s, RBCs and WBCs • ANA often present but not specific. Anti-Smith + in SLE • Anti-double-stranded DNA more specific than ANA. • CH50, C3 and C4 are decreased in active disease • Dx: 4 of 11 criteria, usually ANA positive
Systemic lupus erythematosus • 18 yo woman with multisystem disease and these painless symmetric vasculitic changes on fingers
Systemic lupus erythematosus • Older teen with recent diagnosis of SLE • Characteristic ‘malar’ rash associated with lupus • Also had severe renal involvement • Getting high doses of IV steroids
Meningococcemia • Overwhelming bacterial infection caused by Neisseria meningitidis • Sepsis, meningitis, or both • Onset abrupt with fever, chills, malaise, prostration, and typical rash: “purpura” or “petechiae” • Fulminant cases: purpura, “DIC”, shock, coma, and death within several hours.
Neisseria meningitidis • Can cause meningitis, pneumonia, occult bacteremia, conjunctivitis, chronic meningococcemia. • Invasive disease complications: arthritis, myocarditis, pericarditis, endophthalmitis • 5 groups (A,B,C,Y,W135) • Short incubation period (1-10 days, mostly < 4 d) • Gram stain, cultures from blood/CSF/skin scraping or joint, buffy coat smear; antigen in CSF. • Detectable in CSF by PCR (30-50% + in UK) • Rx: Penicillin, cefotaxime, ceftriaxone, ampicillin • Short courses of treatment are adequate (5-7d)
Neisseria meningitidis meningitis and meningococcemia • Isolation: droplet precautions until 24 hours Rx. • 4-valent vaccines available, not including group B. • Chemoproph with rifampin, ceftriaxone or cipro • Prophylaxis for household contacts, childcare, nursery school contacts within 7 days, direct exposure to patient’s secretions, mouth-to-mouth resuscitation, sleeping/eating close to patient within 7 days of onset of symptoms, and in outbreaks.
Here’s an Easter Bunny in ICU • This bunny was left on the bed of the patient with meningo-coccemia • The boy recovered… • The bunny didn’t!
Nephrotic syndrome: spontaneous bacterial peritonitis • 10 yo girl with long hx of nephrotic syndrome (proteinuria, low albumin, edema, hyperlipidemia) • Sunburn over bikini line ? • Came in with fever, abdominal pain, distension, redness • Each time her paracentesis cultures grew Strep pneumoniae or E. coli; responded well to antibiotics.
Omphalitis: MRSA • 6 wo boy, 3-4 days of fussiness, ‘colic’, then fever 102, pan-cultured • WBC 2.7K… to CHO • Pale, mottled, lethargic • IV fluids, antibx for ‘compensated shock’. ID consulted: “mass” in upper abdomen Pressure over mass: volcanic eruption through umbilicus, caught with dad’s cell phone camera. Further studies: extended into porta hepatis ! I&D done and patient recovered fully with 3 weeks IV abx.
Osteomyelitis, MRSA(Methicillin-resistant Staph aureus) • 13 yo boy had infected toenail, spread up leg to shin, eventually to tibia: cultures grew MRSA • Treated x 6 months with various IV antibiotics • Infection flared every time we tried to stop antibiotics • Boy faced amputation • UCSF Dr. Dyab saved his leg!
Pseudoverrucous papules Girl with HIV and severe diarrhea for several weeks Boy with suprapubic vesicostomy and recurrent UTIs
Pott’s Puffy Tumor • 14 yo boy with swollen, tender forehead • Typical of teenage boys • Often no prior symptoms • CT scan essential to dx • Unrecognized sinus dz • Extension into forehead • CT: epidural abscess ! • Needs drainage! Common organisms: 50% are Strep pneumoniae or H. influenzae; others: viridans Strep, group A Strep, or Staph aureus
Cutaneous larva migrans • 12 month old child from Sri Lanka, nursed x 4 months • Then came to US on 12/15/04 with adoptive parents • Poor weight gain x 3-4 mos • Possible abdom discomfort • 2 weeks prior parents noted red, raised bump near anus, now expanding in linear fashion laterally, then curled in loop • No visible ‘worms’ in stool
Cutaneous Larva Migrans • Nematode larvae produce pruritic, reddish papules at site of skin entry “creeping eruption” • As larvae move, leave intensely itchy serpinigous tracks (~pathognomonic) • Eventually self-limiting (wks-months) • Rare complic: severe pneumonia (Loeffler syndrome), myositis, eosinophilic enteritis.
Cutaneous Larva Migrans • Cat and dog hookworms: Ancylostoma braziliense and Ancylostoma caninum. • Contact with soil contaminated with dog, cat feces • US: Southeast. • Dx: Clinical; +/- eosinophilia; larvae in sputum (pneu); serology not readily available • Rx: No Rx (self-limited) or albendazole, ivermectin or topical thiabendazole
Staphylococcal Scalded Skin Syndrome (SSSS) - Ritter disease • 20 month old, East Indian girl admitted 12 hours ago • High fevers, irritable, intense erythroderma • + Nikulsky, peeling around mouth, red eyes • NP and skin from near rectum both: S. aureus • Gradually recovered on Burow’s soaks, eucerin, vaseline or aquaphor, and pain meds, IV antibiotics
Staphylococcal scalded skin syndrome • Toxin-mediated complication of a • Staph infection (phage gp 2, strains • 71, 55): exfoliative toxins A or B. • Mostly < 3 yo • First malaise, fever, irritability, • exquisite tenderness of skin • Diffuse redness diffusely, worse in • creases and around mouth • Eyes red, purulent, sticky • Skin wrinkles, blisters, erodes. • Sheets peel off (+ Nikulsky sign). • Peels 2-5 days later, heals without • scars. Quick recovery.
Sexually transmitted disease(s)? • 17 yo teen came to ER • Had 10 recent partners and didn’t know names of any of them • Ulcer is painless now • Had swollen, painful, red nodes in groin • Refused HIV testing • GS: gram-neg diplococci • Cx: Group B Strep, • RPR: positive (syphilis) • Suspected: H. ducreyi too H. ducreyi = chancroid, painful ulcer & painful nodes; rx: Azithromycin or cipro GND: Ns. gonorrhea?
Shingles: “Herpes zoster”, caused by Varicella zoster virus (VZV) • Previously well 6 yo came in with low-grade fevers and this blistering rash on L leg • Often no prior history of primary chickenpox (typically unrecognized, kids had it in 1st 12 months) • Typical dermatomal distribution (this is S1) • Usually contagious only with contact with blister fluid.
Shingles: Varicella zoster • 14 yo with perinatally acquired HIV/AIDS • CD4 250 range and HIV viral load 60,000, on “HAART” Rx • Hx 10 varicella 1997 • 2 days left neck pain • Rash emerged over 12-24 hours • C3 dermatome only • Slowly responsive to acyclovir and gabapentin (Neurontin). • Better with higher dose ACV
Stevens-Johnson Syndrome (SJS) • 12 yo with 3 prior episodes of oral erythema multiforme (bx +), last one ‘aborted’ with steroids. No prior skin dz. • Evidence of HSV, mycoplasma with high IgG and +++ IgM • Now flu-like illness, fevers x 1 week, oral swelling, rash over chest, rapidly spreading • Rash worsened, mouth swollen, progressed rapidly overnight • Ended up in ICU
Erythema multiforme vs SJS? • EM: Numerous skin manifestations: macules, papules, vesicles, bullae, urticaria (hives), plaques, confluent erythema (redness) • Most common 10-30 yo, asymtomatic or with some burning, itching; extremitis more than torso, face. • Characteristic lesion is doughnut-shaped, target-like papule with red border and inner pale ring and dusky-to-purple center (like an iris or bull’s eye). • Abrupt onset. • Underlying causes, triggers may vary. • EM minor vs EM major (Stevens-Johnson syndrome)