Download
1 / 24
240 likes | 383 Views
Which types of smokers get which service?. ENQ conference Rome, 10/11 December 2007 Marc Willemsen, Sander Bot, Regina van der Meer. STUDIES (Cost-)effectiveness of quitlines Treatment / service <–> characteristics of callers Quitline tel. on cigaret packs -> call volumes

E N D
Which types of smokers get which service? ENQ conference Rome, 10/11 December 2007 Marc Willemsen, Sander Bot, Regina van der Meer
STUDIES • (Cost-)effectiveness of quitlines • Treatment / service <–> characteristics of callers • Quitline tel. on cigaret packs -> call volumes • HELP campaign -> call volumes
Denmark Germany Ireland Italy The Netherlands Norway Portugal United Kingdom France STOP-Line Counselling German Cancer Research Unit The National Smokers Quitline Lega Italiana per la lotte contro iI tumo STIVORO Directorate for Health and Social Affairs Instituto Nacional de Cardiologia Preventiva) QUIT UK Insititut National de Prévention et d’Education pour la Santé The 9 Participating Quit Lines
ESCHER Objectives • Develop an evidence base for European quitlines • Collect basic data that are usefull for all countries involved and are of interest to the EU • Strengthen the position of the quitlines • Take advantage of natural variation between • countries (compare quitlines in natural settings)
Which smokers get the most effective treatment from quitlines?
Literature sent Booklets or leaflets on quitting Basic information Objective / neutral information about facts, consequences of stopping smoking, craving etc. (quick call) Specific information Objective / neutral information about cessation methods (pharmacotherapy), referral tooutside services or referral to health professional Advice Recommendations on how to quit smoking, eg., what would be the best method to quit or recommendation to see health professional Counselling Caller-centred and person-tailored, in-depth, motivational interaction Type of treatment
Hypotheses • 1. Heavy smokers more likely to receive counselling + get specific info on pharmacotherapy • 2. Lower educated callers more likely to receive counselling, less likely to receive brief advice or written materials • 3. Callers in action stage more likely to get counselling or advice, less likely to be referred to outside help • 4. Referred callers more likely to get counselling
Method • In each country, during a period of 12 months (February 2005 – April 2006) up to 500 smokers were recruited. • Subjects: “every caller who calls for telephone support for smoking cessation”. • Data collected by the counsellors during the first contact (intake). • Logistic regression, controlling for country. Method = enter 7 services. Check country x treatment interactions.
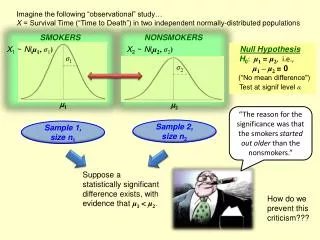
Heavy smokers (HSI >=3) • No association with counselling (contrary to hypothesis) (75% vs. 78%; ns) • More likely to get information about pharmacotherapy (OR=1.27; 95%CI=1.10-1.47) (hypothesis confirmed) • More often referred to a health professional (OR=1.32; 95CI=1.08-1.60). • Consistent across 9 quitlines
Low education callers Not more likely to receive counselling (hypothesis rejected) No relationship with receiving brief advice or written materials. (hypothesis rejected).
Low educated • More information on pharmacotherapy • (OR=1.18; 95%CI =1.01-1.38) • Consistent across 9 quitlines
Low educated: shorter calls • Percentage having a ‘long call’ • (>20 minutes)
Action stage • More likely: • Advice1 • Counselling 2 • (Hypothesis confirmed) • 1 French, German, Irish quitlines; • 2 Italian, Dutch quitlines
Action stage • Less likely: • Referral to outside help3 (hypothesis confirmed) • Referral to health professional4 • 3 Danish, German, Italian, Portuguese, English quitlines; • 4 Irish, Portuguese
Callers referred by a health professionalcompared to other referrals • Heavy smokers (53% vs 43%) • Low educated (35% vs 29%)
Callers referred by a health professional • More likely get counselling (hypothesis confirmed) (81% vs 74%) • More likely information on pharmacotherapy (50% vs 38%) • Less likely brief advice (48% vs 54%) and literature (41% vs 49%) • All quitlines, except Danish, French, English (in these countries: more likely to be further referred to medical professional: 38% vs 10%).
Conclusions • The most effective quitline service (counselling) was provided to higher educated smokers, callers in action stage of change, and callers who were referred by a health professional. • Callers who were referred by a health professional more likely to be low educated and heavy smoker • Although many low educated callers received information about pharmacotherapy, low educated smokers came of badly in terms of counselling (less likely + shorter calls).
Conclusions • In contrast to the US and Australia, in these nine European quitlines, only 10% of contacts were referrals from health care providers. • European quitlines should be better integrated into the health care system.
Thanks for your attention! • Contact: mc.willemsen@stivoro.nl