Download
1 / 16
180 likes | 315 Views
Group 3 : Fibular Hemimelia. Alina Bodea – Co Presenter & Writer Farley Bouguillon - Writer Ravneet Singh - PowerPoint William “Tim” Wells - Presenter Yunes Ahmed – PowerPoint Chasity Lorenzo – Research Julia Lee – Research. What is Fibular Hemimelia?

E N D
Group 3 : Fibular Hemimelia Alina Bodea – Co Presenter & Writer Farley Bouguillon - Writer Ravneet Singh - PowerPoint William “Tim” Wells - Presenter Yunes Ahmed – PowerPoint Chasity Lorenzo – Research Julia Lee – Research
What is Fibular Hemimelia? • Fibular hemimelia is a birth defect where part or all the fibular bone is absent. • Most often it is unilateral. • Diagnosis and Causes • Can be observed when scans are done during pregnancy. • Shortened leg, ankle or knee instability due to absence of fibula bone. • Most cases of fibular hemimelia are thought to occur for no particular reason.
Patient History • A seven year old female patient was scheduled at Columbia Presbyterian Children Hospital for a follow up appointment. • At birth, she was diagnosed with fibular hemimelia of her right lower extremity. • She had begun a right tibial lengthening process at the age of one.
Fibular Hemimelia Types Type 1: Short or partial proximal absence unilaterally 1A: Stable ankle joint ± ball & socket joint with mostly medial tilt. 1B: Unstable ankle joint where the proximal fibula is reduced 30-50% of its normal length.
Fibular Hemimelia Types Type 2: Complete absence of the Fibula • Can be unilateral or bilateral. • Tibia can be extremely small and bowed with proximal femoral focal and upper limb deficiency.
Fibular Hemimelia Distal Femur AP Tibia View Tibia Lengthening
Treatment • Treatment will depend on the severity and condition of the limb. • Choices consist of either amputation of lower leg or tibia lengthening. • Tibial lengthening was the preferred treatment method used in this case.
Views Ordered and Obtained • AP, oblique, and lateral views of the right ankle. • AP and lateral views of the right tibia and fibula. • 3 joint right lower extremity exam.
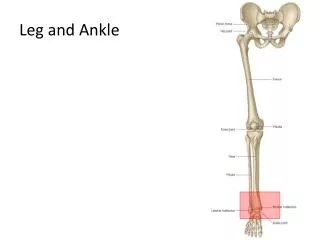
Anatomy and Physiology of the Ankle • The ankle is made up of two joints: the ankle and the subtalar joint. The ankle joint includes two bones (the tibia and the fibula) that form a joint that allows the foot to bend up and down. • Two bones of the foot (the talus and the calcaneus) connect to make the subtalar joint that allows the foot to move side to side.
Anatomy and Physiology Lower Leg • The tibia is a long bone of the lower leg, found between the patella and the ankle. • The fibula is a long, thin bone running parallel to the tibia. • Like the femur, the tibia bears much of the body’s weight and plays an essential role in movement andlocomotion.
Positioning and Techniques • For the ankle examinations, the patient was supine with leg extended. For the AP and oblique views the foot was dorsiflexed foot 90°, the central ray was perpendicular to the ankle joint at a point midway between the malleoli. The oblique view was obtained by medially rotating the foot 15-20 degrees. • For the lateral view, the patient turned toward the affected side, until the leg was laying lateral along the table, placing the patella perpendicular to the IR, dorsiflexing the foot and directing the central ray perpendicular to the ankle joint, entering the medial malleolus. • The technique utilized for the ankle exams was 55 Kvp and 4 mAs at an SID of 40 inches.
Positioning and Techniques • The lower leg projections required the patient to remain in the supine position for the AP view, adjusting the femoral condyles so that they would be parallel to the IR with the foot dorsiflexed. The central ray was perpendicular to the mid shaft of the lower leg. • The lateral projection was obtained by turning the patient onto the affected side with the femoral condyles perpendicular to the IR. • The technique necessary for the lower extremity views was 55 Kvp at 4 mAs with an SID of 40 inches.
Positioning and Techniques along with Equipment • For the 3 joint lower extremity projection, the patient was standing erect in the AP position, feet shoulder width apart and collimation was opened to the level of the iliac crest down to the ankle joints. • The technique used for the 3 joint lower extremity view was 60 Kvp and 5 mAs at an SID of 60 inches. • No contrast medium is necessary for these projections, as the anatomy of interest is bone. • Proper shielding was used with a Philips digital imagingsystem in all exams.
Radiographic Findings • A solitary bone of the right lower leg. • Left femur was approximately 11 millimeter longer than the right femur. • Left tibia arises 2 centimeter higher than the right tibia. • Distal right tibia epiphysis was absent or dysplastic. • Wire hardware seen in the right proximal tibia.
Conclusion • A young girl who at birth presented with the condition of fibular hemimelia. • Surgery was performed at the age of one year in order to install the external fixator device so as to gradually lengthen the tibia. • There will be an indeterminate number of follow up surgeries along with radiographic exams to both monitor and visualize the progress, until the expected outcome is achieved.
References: • Merrill’s Atlas of Radiographic Positioning • S.Viquet, Carrin P.Garnero,P.D.Delmas- The role of collagen in bone strength • Peter G. Bullough –Fibular Hemimelia • Medicinenet.com • Springer.com- Clinical Orthopedics and related research • ethanfgodschild.blogspot.com- God's Warrior~ Fighting Fibular Hemimelia • sportsmedicine.about.com - Ankle Anatomy and Physiology • wikiradiography.com • boundless.com-Tibia and Fibula (Leg)