Download
1 / 20
240 likes | 1.2k Views
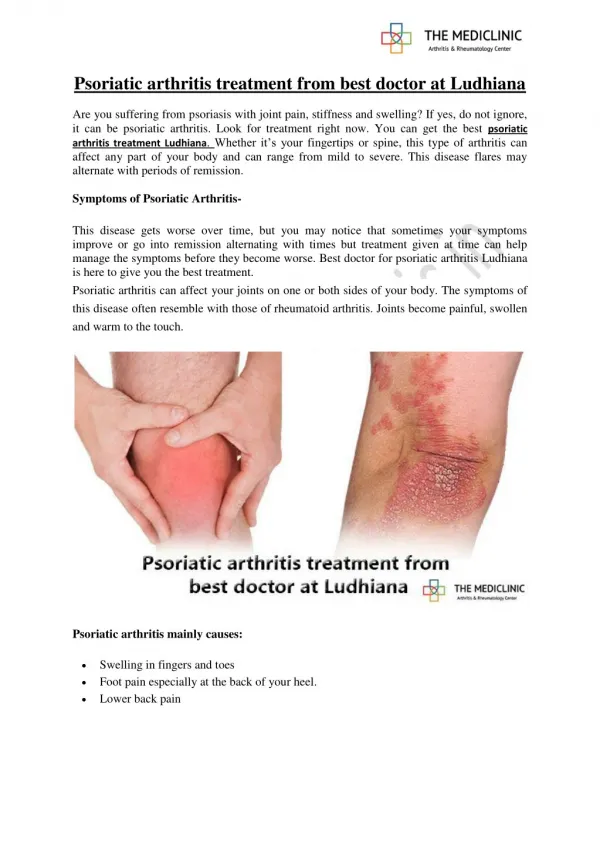
Psoriatic arthritis. DIP joint Involvement Nail changes. Psoriatic arthritis. Nail pitting in psoriatic arthritis. Psoriatic arthritis. Deforming arthritis. Psoriatic arthritis- pseudorheumatoid. Looks like RA But RF – psoriasis. What is this diagnosis?. Osteoarthritis.

E N D
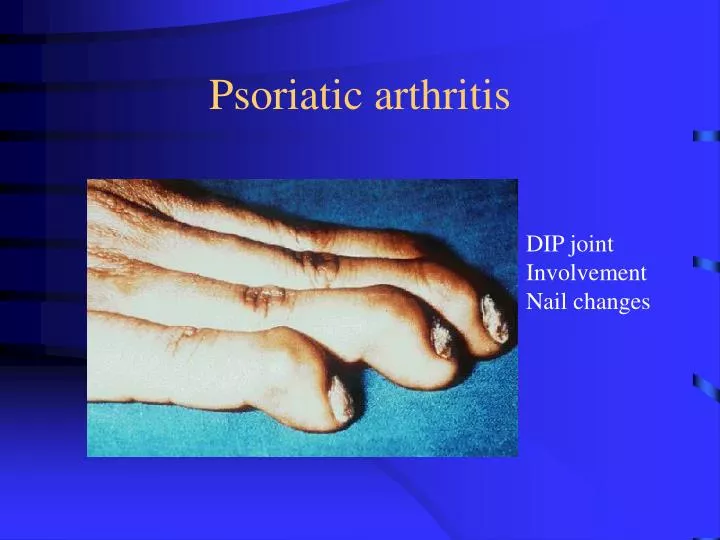
Psoriatic arthritis DIP joint Involvement Nail changes
Psoriatic arthritis Deforming arthritis
Psoriatic arthritis- pseudorheumatoid Looks like RA But RF – psoriasis
What is this diagnosis? Osteoarthritis
What is this diagnosis? Osteoarthritis
Beware the rare but serious…. • Conditions that may present with inflammatory arthritis like RA • Polymyositis, dermatomyositis: should have muscle weakness, RF can be + low titre, do CK • Vasculitis eg Wegener’s granulomatosis: always do U/A, renal function, RF-, ANCA +, may be very resistant to usual RA therapy • Neoplastic conditions: resistant to usual RA therapy
Case history 5 • 25 year old man, episode of diarrhoea, 3 weeks later onset of knee swelling, followed by ankle swelling and achilles tendonitis • Unable to walk in mornings due to pain and stiffness • By midday joints “warmed up” • No conjunctivitis, no dysuria, diarrhoea settled, no rash
Investigations • FBC normal • ESR 53, CRP 36 • UEC normal • RF negative • ANA negative • Stool cultures- negative
Clinical picture Left knee effusion
Diagnosis • Sero-negative inflammatory arthritis reactive arthritis • Think of this group if past history of diarrhoea (eg salmonlla), dysuria (eg chlamydia), sore throat (strep) • Typical joint distribution: lower limb asymmetrical, knee, ankle, enthesitis with achilles tendonitis, plantar fasciitis, sausage toes (dactylitis)
Case history 6 • 35 year old man • 3 year history of low back, buttock pain • Worse in the morning, improves with walking around. • Wakes him in early hours of the morning • Past history of red eye many years ago, treated with steroid drops
Examination and investigations • No peripheral joint synovitis • Back movements: some limitation of lumbar flexion, nil else • FBC normal • ESR, CRP normal • Diagnosis? • Further investigations?
Diagnosis • Inflammatory back pain • Sero-negative spondyloarthropathy • Do pelvic Xray to look at sacro-iliac joints • HLA-B27 antigen • Not diagnostic test for ankylosing spondylitis • 10% normal population HLA-B27+ • 90% AS HLA-B27+
Psoriatic arthritis Ankylosing spondylitis subtype
Joint distribution • Symmetrical, small joint arthritis, MCP, PIP, wrists, MTPs +/- other joints • Think RA, psoriatic, SLE or viral • Asymmetrical, predominantly lower limb, ankle knee, enthesitis • Think sero-negative spondyloarthropathies • Psoriatic, Reactive, ankylosing spondylitis • Sacro-iliac (buttock) pain, spinal stiffness • Think sero-negative spondyloarthropathies, eg ankylosing spondylitis