Download
1 / 23
250 likes | 269 Views
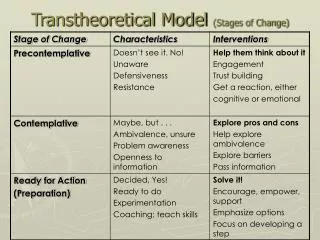
Systems of Psychotherapy: A Transtheoretical Analysis. Chapter 8. Exposure Therapies. Implosive Therapy. Thomas Stampfl (1923 – 2005) Basic tenets Learned Avoidance : reduces anxiety in the short term Generalization : avoidance of similar situations

E N D
Systems of Psychotherapy:A Transtheoretical Analysis Chapter 8. Exposure Therapies
Implosive Therapy • Thomas Stampfl (1923 – 2005) • Basic tenets • Learned Avoidance: reduces anxiety in the short term • Generalization: avoidance of similar situations • Extinction: gradual disappearance of conditioned anxiety due to lack of reinforcement • While implosive therapy pioneered the confrontation of fear, it is less popular today than exposure therapies
Exposure Therapies • Directly confront feared stimuli & activate intense emotions • Particularly useful in tx of anxiety & trauma • 2 exposure therapies in chapter • Exposure (Edna Foa) • Eye Movement Desensitization & Reprocessing (EMDR) (Francine Shapiro)
A Sketch of Edna Foa • Born in Israel in 1937 • Spent most of career in behavior therapy • Collaborated with colleagues in examining exposure therapy for anxiety disorders • Premier proponent of prolonged exposure (PE) with response prevention (RP) • Recently has been disseminating and implementing PE+RP -
Theory of Psychopathology • Anxiety is conditioned response controlled by respondent learning & operant learning • Conditioning accounts for acquisition & extinction of fear • Conceptualizes psychopathology in terms of both behavioral & emotional processing
Prolonged Exposure • Intensive (direct & immediate) vs. gradual (slow & incremental exposure) • Imaginal (imagining fear stimuli) vs. in vivo (actual place or tactile material) • Total vs. partial response prevention
Therapeutic Processes • Clients given clear treatment rationale • Taught anxiety coping skills • Prolonged exposure • Given homework • Maintenance sessions as needed
Therapeutic Relationship • Exposure therapist acts like an effective, firm parent • Clients’ trust of therapist allows them to stay in presence of feared stimuli • Therapist models confidence
Practicalities of Exposure Therapy • 8 – 12, 1 to 2 hour sessions • Homework assigned • Training widely available from behavior & cognitive therapists • Therapists must address their own anxieties
Effectiveness of Exposure Therapy • Effective in treating PTSD, OCD, specific phobias, & social phobia • Proves superior to psychoactive medications alone for treating PTSD • Only small % of clients experience symptom exacerbation • Low relapse rates but high refusal rates • Treatment of choice for many anxiety disorders
A Sketch of Francine Shapiro • Cancer diagnosis led to her search for solutions to its psychological effects • Discovered deliberate eye movements made her thoughts less distressing • Founder of EMDR & EMDR Humanitarian Assistance Program • Controversial early on for restricting EMDR training
Theory of Psychopathology • Psychopathology occurs when information processing is blocked • Trauma is trapped or locked in the neurophysiology • Everyday stimuli trigger re-experience of traumatic event
Therapeutic Processes • Adaptive information processing (AIP) model • Counterconditioning via desensitization, distancing, & cognitive restructuring • Consciousness raising & catharsis operate, but not as central mechanisms
Phases of EMDR • Client history • Preparation • Desensitization • Installation • Body scan • Closure
Therapeutic Relationship • Characterized by empathy, trust, & safety • Clinicians communicate respect for client courage, but not during active processing • Safe haven created through rapport, teaching relaxation, and “stop signal”
Practicalities of EMDR • Typically 4 to 6, 90-minute sessions • Two weekend workshops & supervised practice to acquire competence • Providing pro bono treatment & training in disaster areas
Effectiveness of EMDR • As effective (and typically briefer) as exposure and CBT methods for trauma • Two systematic reviews conclude that EMDR may be promising option for chronic pain • Meta-analysis indicates the eye movements may account for some of EMDR’s power • Remains controversial despite large research base
Criticisms of Exposure Therapies • From a Cognitive-Behavioral Perspective (no need to create a new school of therapy) • From a Psychoanalytic Perspective (reducing phobia is insufficient, trauma is not resolved) • From a Humanistic Perspective (artificially evoked emotion, lack of therapeutic relationship) • From a Cultural Perspective (treat the social causes, not symptoms, to prevent the trauma) • From an Integrative Perspective (need to identify the active ingredients)
Future Directions • Implosive therapy losing popularity • Exposure on the rise for intransigent anxiety-based disorders,becoming more integrative • Virtual reality exposure gaining popularity • Future of EMDR is not clear, but research will compare processing methods (eye movements, hand taps)
Key Terms adaptive information processing avoidance conditioning/learning avoidancerepression (cognitiveavoidance) breathing retraining classical/respondent conditioning clinical significance (vs. statistical significance) cognitive interweave cue exposure desensitization phase dismantling studies emotional processing theory exposure therapy extinction Eye Movement Desensitization & Reprocessing (EMDR) generalization habituation
Key Terms (cont.) imaginal exposure implosive therapy in vivo exposure installation looping neurotic paradox operant/instrumental conditioning pro bono prolonged exposure response prevention subjective units of distress (SUD) symptom exacerbation treatment fidelity two-factor theory of learning (Mowrer’s) Validity of Cognition (VOC) scale virtual reality exposure
Recommended Websites • Center for the Treatment and Study of Anxiety (Foa): www.med.upenn.edu/ctsa/ • EMDR Institute: www.emdr.com • EMDR International Association (EMDRIA): www.emdria.org/ • International Society for Traumatic Stress Studies: www.istss.org/ • Virtual Reality Exposure Therapy: www.virtuallybetter.com