Download
1 / 31
310 likes | 541 Views
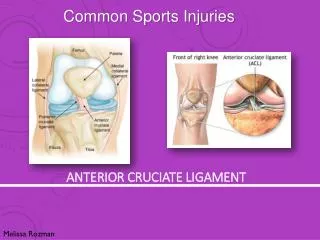
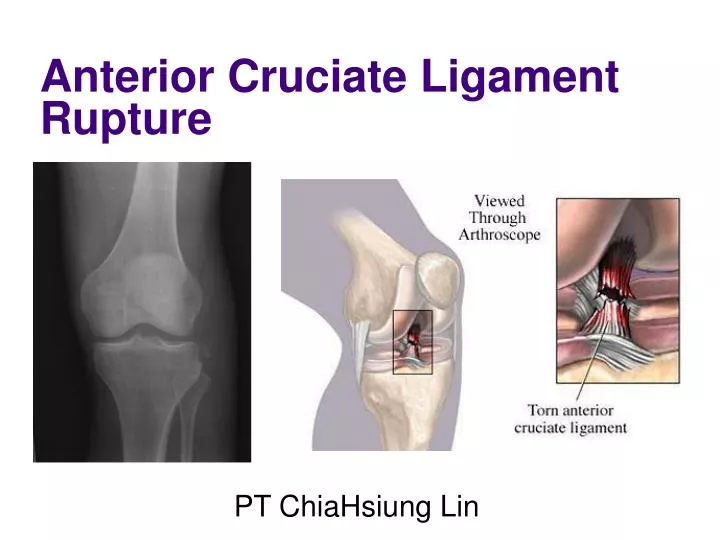
Anterior Cruciate Ligament Rupture. PT ChiaHsiung Lin. Anatomy. Functional Anatomy. Anterior tibial plateau to the posterior femoral intercondylar notch The tibial attachment is to a facet, in front of, and lateral to the anterior tibial spine.

E N D
Anterior Cruciate Ligament Rupture PT ChiaHsiung Lin
Functional Anatomy • Anterior tibial plateau to the posterior femoral intercondylar notch • The tibial attachment is to a facet, in front of, and lateral to the anterior tibial spine. • The femoral attachment is high on the posterior aspect of the lateral wall of the intercondylar notch. • The biomechanical function of the ACL in its stabilizing role it has four (main) functions: • 1. Restrains anterior translation of the tibia; • 2. Prevents hyperextension of the knee; • 3. Acts as a secondary stabilizer to valgus stress, reinforcing the medial • collateral ligament; • 4. Controls rotation of the tibia on the femur in femoral extensions of 0-30°.
Causes of ACL Rupture ~ A traumatic force being applied to the knee in a twisting moment. ~ With either a direct or an indirect force. i.e., while side-stepping, pivoting or landing from a jump. ~ associated with some type of contact, whether it be on the football field, on the snow fields or in a motor vehicle accident.
# Hyperextension knee is straightened more than 10 degrees beyond its normal fully straightened position # Pivoting injuries of the knee with excessive inward turning of the lower leg can also damage the ACL.
*About 40% of all individuals experience a "popping" sensation at the time of the injury,which may also produce a tearing sensation. * Most ACL injuries occur during athletic activity. Often those are non-contact activities with the mechanism of injury usually involving: • Planting and cutting : turning one direction or the other. Example: Football or baseball player making a fast cut and changing direction. • - Straight-knee landing : results when the foot strikes the ground with the knee straight. Example: Basketball player coming down after a jump shot or the gymnast landing on a dismount. - One-step-stop landing with the knee hyperextended : results when the leg abruptly stops while in an over-straightened position. Example: Baseball player sliding into a base with the knee hyperextended with additional force upon hyperextension. - Pivoting and sudden deceleration resulting from a combination of rapid slowing down and a plant and twist of the foot placing extreme rotation at the knee. Example: Football or soccer player quickly slowing down followed by a quick turn in direction.
Mechanism of injury • * Approximately 80% of injuries occur in non-contact situations when landing from a • jump or during deceleration and change of direction on a fixed foot. • * If no other player is involved, this means the athlete is placing his or her own leg in a • vulnerable position. • * The ‘Position of No Return’ is the movement combination that most often • leads to ACL rupture. • Suspicious of ACL Rupture? • The following signs and symptoms are often associated with ACL rupture • a bad landing from a jump or decelerating and twisting injury. • Immediate pain and swelling. Usually, when the ACL is torn, it bleeds and fills the knee with blood. • A sensation of giving way or instability
Examination * Palpating (feeling) the knee allows an assessment of swelling and inflammation - an inflamed knee may be very hot and tender as well as swollen. * The examiner will ask you to bend and straighten the knee as far as you can, he may then add some overpressure at the limits of your movement to check the full range. Any block to movement or pain will be noted as significant. * Typically your doctor or physiotherapist will test for cruciate ligament damage by assessing how far the tibia will glide forwards and backwards on the femur. * Usually he will test both legs and compare them - this is because there is a natural difference in normal movement between different people, the examiner will use your uninjured leg to represent what is normal for you.
Clinical Assessment Standing leg alignment and varus thrust in gait Assess hyperextension of opposite knee Lachman Test Tip- feel the end point whilst performing the Lachman test. • Pivot Shift Test • Tip - Start the pivot shift test from full extension and apply slight axial force in addition to valgus • and internal rotation.* Check Posterior sag tibia (PCL) as it can lead to a wrong diagnosis of ACL injury.* Check collateral stability- missed lateral ligament injury can be a reason of ACL reconstruction • failure. (MRI scans or Arthroscopy are not needed for routine diagnosis of ACL rupture).
Testing for the ACL is done with your knee bent approximately 20-30° from the horizontal. This test is called the Lachman test and is very sensitive and specific for the ACL. Testing for the PCL (posterior cruciate ligament) is done with the knee bent at 90° and is called the 'Drawer test'. Lateral pivot shift test. This involves applying a sideways pressure on the joint while rotating and bending it however, it can be difficult to perform in an acute situation or if a patient is very tense. It is more likely to be tried when examining a more chronic injury, or if assessing a joint under anaesthetic.
Further diagnostic testsOther investigations may prove necessary. Further diagnostic tests may be indicated to confirm a questionable diagnosis or to check if any other structures have also been injured - this could affect the treatment required. A Standard X-ray This will only show bone but it may be important to rule out any fractures (breaks) and also to see how the bones are positioned in relation to each other. Sometimes a 'stress X-ray' is done to assess the integrity of the collateral ligaments - the X-ray is taken while sideways pressure is applied to the knee.
An MRI Scan This will show all the structures in the knee and enables a reliable diagnosis to be made however, scans are very expensive and are not always available or if they are, there may be an unacceptably long wait. • The first image demonstrates an intact cruciate • ligament. B. The second image demonstrates a torn ACL.
Findings: Anterior drawer sign (lateral tibial plateau > 5 mm relative to retrofemoral line); Buckled PCL sign (tangential line along posterior margin of PCL doesn't intersect distal femur); LCL seen almost entirely on a single coronal image (due to anterior subluxation of tibia).
Management of the Ruptured ACL Treatment for an Anterior Cruciate Rupture What can the athlete do? • Immediately stop play or competition • Apply RICE (Rest, Ice, Compression, Elevation) to the knee immediately • Seek medical attention as soon as possible. • Once the diagnosis of ruptured ACL is made, management can be divided into conservative and surgical. Correct choice of treatment depends on assessment of three patient factors: • • Age • • Functional disability • • Functional requirements
Operative Treatment Timing • Timing of surgery can affect postoperative recovery of range of movements dueto arthrofibrosis. Too delayed a reconstruction (>12 months) can result in higher meniscal injuries and degenerative changes (Keating 2005). • Factors affecting timing of surgery are • 1. Associated ligamentous and/or meniscal injuries • 2. Preoperative condition of the knee- minimal or no swelling, minimal warmth, • good strength, leg control and range of movements and preferably • symmetrical extension • 3. Mental preparation of the patient/school/ work/holidays. Graft choice The main choices for graft for current day ACL reconstruction are • Autologous- Hamstring, Patellar tendon, quadriceps tendon • Allograft- Patellar tendon, Hamstring, Achilles tendon
Decision on SurgeryThe fundamental reason for surgical treatment is to stop symptomatic instability which can produce recurrent injury- especially meniscal tears. Not all patients with ACL rupture have this instability pattern.This is because poor results from ACL reconstruction can often be due to presence of significant meniscal and chondral injuries from chronic instability. Hence it is important to know that a trial of rehabilitation is not a routine for all ACL injuries. Tibial avulsion Left: Normal knee MRI ACL and PCL . Right: ruptured ACL
Tunnel position and the isometric point • Success of ACL reconstructions depend primarily on achieving proper tunnel position and graft fixation followed by appropriate rehabilitation. Malposition of tunnels can produce restricted movements, increased laxity or graft failure secondary to impingement. There is no isometric point for the tibial tunnel. Both tunnels have to be made within the anatomical foot print of the ACL. * Landmarks for tibial tunnel 1. Posterior aspect of the tibial ACL footprint 2. About 7mm anterior to the PCL with the knee flexed 90 degrees 3. Between the tibial eminences 4. Just posterior to the posterior edge of the anterior horn attachment of the lateral meniscus 5. About 43% posterior to the anterior edge of the tibia along the length on the sagital plane of the tibia 6. The oblique orientation of the tibial tunnel in the coronal plane (about 60-70 degrees) is important for transtibial drilling of femoral tunnel. This means that the entry point on the tibia is close to or sometimes through superficial MCL.
Landmarks for femoral tunnel • 1. The ACL femoral insertion has a length of 18mm width of 10mm and is 4 mm from the posterior articular cartilage. The tunnel has to be within the lower part of this footprint • 2. With the knee flexed 90 degrees and imagining the femoral tunnel position as the face of a clock, the aperture should be at 10-11 o’clock for the right knee and 1-2 o’clock for the left knee. • 3. Femoral tunnels can be drilled transtibial or through the medial portal. For anteromedial portal technique the knee should be flexed about 120 degrees to avoid damage to the lateral structures. For transtibial technique, the tibial tunnel has to be perfect and the knee is flexed 90 degrees • 4. A 5 or 6mm offset femoral guide is placed in the over-the-top position and the jig rotated slightly to achieve more lateral femoral tunnel aperture. • 5. To achieve more flexibility in tunnel positioning, the antero-medial portal can be used or the femoral tunnel can be drilled free hand via the tibial tunnel through a tunnel plug
Graft fixation • The options for fixation of any graft are - • 1. Interference screw fixation- RCI screw, Softsilk, Bioscrew, Milagro • 2. Cortical fixation- Endobutton, WasherLoc/EZloc, Sutures over button • 3. Suspensory fixation in the aperture- Crosspin, Rigidfix • In general cortical fixation gives the best strength. When screws are used they have to cortico-cancellous- not purely cancellous. Over sizing screw diameter by 1mm or longer screw increases fixation strength. Concentric screw placement gives superior fixation strength compared to eccentric screw placement (Starch, Gwynne-Jones).
Rehabilitation • Anterior cruciate ligament rehabilitation has undergone considerable changes over the past decade. Intensive research into the biomechanics of the injured and the operated knee have led to a movement away from the techniques of the early 1980's characterized by post operative casting and delayed rehabilitation, to the current early rehabilitation program. • * The major goals of rehabilitation following • ACL surgery are: • • restoration of joint anatomy; • • provision of static and dynamic stability; • • maintenance of the aerobic conditioning and psychological well being; and • • early return to work and sport. • These have required the development of an intensive rehabilitation program in which the patient has to take an active involvement.
* The graft is weakest between six and twelve weeks post operatively so programs must be designed to protect the graft during this period. On the other hand investigations into ligamentous healing have shown that progressive controlled loading provides a stimulus for healing which improves the quality of graft incorporation. * More over, early immobilization has advantages such as maintenance of articular cartilage nutrition and retention of bone mineralization. * Kinematic research has shown quadriceps contraction causes greatest strain on the anterior cruciate ligament graft between 10° and 45° of flexion. The anterior cruciate ligament graft lacks the normal mechanoreceptors that provide biofeedback in the uninjured knee. All these factors must be taken into account when designing rehabilitation programs.
* Accelerated rehabilitation program is divided into four phases. 1. In the first one to two weeks the aims of therapy are to decrease pain and swelling, and increase the range of motion of the knee. A post-operative brace is ranged from 30 to 90° and is used until there is adequate quadriceps control. Physiotherapy including CPM is used immediately post operatively. In this early phase there is an emphasis on static contraction of the hamstrings and co-contractions of the hamstrings and the quadriceps. Crutch -walking with partial weight bearing is allowed and the usual modalities are used to reduce pain and swelling.
2. During the second phase, from two to six weeks, the emphasis is on increasing the range of motion, increasing weight bearing and gaining hamstring and quadriceps control. The patient is usually out of the brace by the third to fourth week. During this phase gait re-education and static proprioception exercises commence. This may include balancing on the affected leg, biofeedback techniques and pool work to maintain conditioning and range of motion.
3. During the third stage, from six to twelve weeks, emphasis is placed on improved muscular control, proprioception and general muscular strengthening. Proprioceptive work progresses from static to dynamic techniques including balance exercises on the wobble board and eventually jogging on a mini-tramp. The patient should have a full range of motion during this stage and gentle resistance work should be added. By the end of this period the patient should be able to cycle normally, swim with a straight leg kick and be able to jog freely on the mini-tramp.
4. The fourth phase of rehabilitation from twelve weeks to six months involves the gradual re-introduction of sports specific exercises aimed at improving agility and reaction times and increasing total leg strength. * An elite athlete who has had a technically well performed early reconstruction of the anterior cruciate ligament followed by an adequate and successful rehabilitation program, should be able to return to the field of his chosen sport between six and nine months.
Rehab after surgery CPM' (continuous passive movement) machine in the early stages Quadriceps bracing : with your legs straight out in front of you, pull your toes up towards you from the ankle and tighten the thigh muscle as hard as you can. Hold for a count of 10 and gently relax.
Flexion : with your legs out in front of you, gently bend your knee, sliding your heel up towards you. You can hold under your thigh and lift to assist the movement initially if you wish but do not lift the heel. There is no restriction to the amount of bend and the sooner it bends fully the better, aim for 90º by the end of the first full day after surgery. Extension stretch : sit or lie with your leg elevated and rest your heel on something at least the same height or preferably higher than your chair (a footstool, coffee table or the arm of the settee!). Let your leg relax so that gravity will help to bring the knee back fully straight. You may only be able to tolerate this position for a couple of minutes initially, (especially if you have had a hamstring graft) that is OK, it will get slightly easier each time you do it. Gradually build up to 10 minutes and repeat this 5/6 times a day. Once you can do this for the full 10 minutes, it is a good idea to do the quadriceps bracing while in this position. Let the leg relax for a few minutes then do 10 braces, then relax for the rest of the stretch time.
Early Progressions at Home As you become more confident moving around you can add to your exercises but be aware of any increase in swelling. Adduction - Lie on your operated side with the opposite leg flexed and behind. Keeping your ankle flexed and your knee straight, lift the operated leg 6 inches off the floor, hold and lower, repeat 5 times then rest. Build up to 6 sets of 5. Knee flexion - use a strap around the foot to gently pull to increase the bend. You can also use an elastic exercise band to push against, to straighten the knee. Abduction - Lie on your side with your operated leg uppermost. Bend the lower leg so that you are balanced. Keeping your ankle, hip and shoulder in line (do not let your hip roll back or bring your leg forwards), lift your leg and lower - repeat 10 times then rest the leg and repeat. Build up to 5 sets of 10.
Bridging - lie with your knees bent and your feet flat. Keeping your stomach muscles tight, lift your hips clear of the floor, hold for a few seconds and gently lower. Begin with 10 repetitions. Extension stretch - you have already done this in sitting, this is another method which is effective. Lie on your front with your legs overhanging the end of the bed, so that your knees are just over the edge. Just relax in this position for 5-10 minutes. If you have a very soft bed, you can place a small rolled-up towel under your thigh to support it. Assisted flexion - Lie on your front. Gently bend your knee, bringing your foot up behind you. Use the opposite leg to assist in the early stages, particularly if you have had a hamstring graft. You may find that you need to assist to initiate the movement but once started you can manage. The aim is to gradually increase the amount of bend, but also to encourage the hamstring muscles to work.
Progressions (day 10 onwards) Aims at this stage: • Restore normal gait pattern • Regain full range of flexion and extension (hopefully you already have this) equal to your opposite knee • Restore normal balance and co-ordination (motor function) • Improve muscle strength, endurance and timing • Progress functional activities