Download
1 / 46
460 likes | 504 Views
Explore the development of female reproductive organs from embryonic stages to pathologies, covering ovarian stroma, mullerian ducts, endometrium, and common infectious diseases. Learn about HPV, herpes, Chlamydia, gonorrhea, and more.

E N D
Embryology • The mesoderm of the urogenital ridge gives rise to the ovarian stroma, just as it does for the Sertoli and Leydig cells of male embryos. • Primordial germ cells from the yolk sac migrate to the ovarian (or testicular) stroma. • Some of these end up in other midline structures, explaining why "germ cell tumors" arise in the retroperitoneum, pineal, and anterior mediastinum.
In female embryos, the mullerian (paramesonephric) ducts result from infolding of the coelomic lining epithelium. • They give rise to the surface epithelium of the ovaries, and the lining of the oviducts and uterus. • In male embryos, Mullerian inhibitory substance from the testis makes the mullerian ducts regress. • In female embryos, the wolffian (mesonephric) ducts regress, persisting only as little bits of epithelium along the whole female tract. • These give rise to "Gardner's duct cysts" along the cervix and vagina. • In male embryos, the wolffian (mesonephric) ducts become the epididymis and vas.
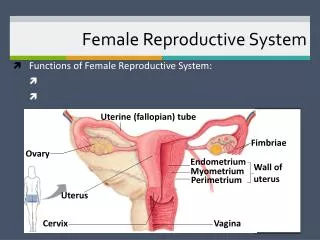
Anatomy and physiology • The outer portion of the cervix ("portio vaginalis") is covered with a thick, nonkeratinizing, stratified squamous epithelium. • The endocervical canal is lined by a simple columnar mucus-producing epithelium. • The squamocolumnar junction usually is located at the bottom of the endocervical canal. • It's near this junction that cancers start ("the transformation zone“).
In young adult women, the endocervical cells may extend out onto the outer surface of the cervix. • This is miscalled an "ectropion" or "erosion"; actually it's normal. • The cervical os is almost entirely closed if a woman has never given birth, and is slightly widened and perhaps fishmouthed if she has.
Only the upper two thirds of the endometrium ("the functionalis") cycles. • The basal third ("the basalis") does not respond to a woman's steroid hormones and stays in place, giving rise to next month's endometrium.
During reproductive life, every month several follicles mature as graafian follicles. • One ovulates and suppresses the others, and becomes a corpus luteum, which will regress when the pregnancy ends or does not occur. • It will be recognizable for a few months, gradually being replaced by scar tissue. • The oviduct's mucosa has ciliated cells, secretory cells, and almost-no-cytoplasm "peg cells" ("intercalated cells"). • The oviduct's mucosa is thrown up into complicated folds ("plica", or "fimbria" at the end).
Herpes Simplex II • Vulva, vagina, cervix: Herpes blisters • Appear 3-7 days after exposure • Pain • Then the little blisters and the systemic syndrome • fever, viral meningitis • The blisters heal in a few weeks but are prone to recur. • Classic "herpes cell" seen on Tzanck preparation or pap smears. • Cells with multiple gigantic nuclei, usually bearing a central inclusion, are diagnostic. • If herpes is transmitted to the child during birth, • severe sickness, brain damage, and even death are likely to occur.
Human Papilloma Virus (HPV) • Vulva: • warts, • intra-epithelial neoplasia, • carcinoma • Vagina and (especially) cervix: • intra-epithelial neoplasia, • carcinoma, • less often warts.
Molluscum contagiosum • Vulva: Molluscum lesions. • This is not necessarily a sexually transmitted disease.
Chlamydia trachomatis • Vulva • Bartholin gland abscess, bad strains can produce lymphogranuloma venereum • Cervix • "Follicular cervicitis", with germinal centers. • Endometrium • "Chronic endometritis", with plasma cells. • Oviduct • Acute / chronic salpingitis ("pelvic inflammatory disease").
Gonorrhea • Vulva • Inflammation and abscesses of Skene's or Bartholin's glands • Vagina • Cervix • Purulent cervicitis. • Endometrium • Endometritis, either acute (with neutrophils) or chronic (with plasma cells) • Oviduct • Acute/chronic salpingitis ("pelvic inflammatory disease").
Hemophilus ducreyi • Vulva • Chancroid Treponema pallidum (syphilis) • Vulva, vagina, cervix • Chancre (primary), condyloma latum (secondary)
Mycobacterium tuberculosis • Oviduct, endometrium TB Calymmatobacterium – Klebsiella granulomatis • Vulva • Donovoniasis, or "granuloma inguinale".
Gardnerella • Vagina: • Nonspecific vaginitis / "bacterial vaginosis" • The bacterium is normal flora; it grows best in the presence of semen but no woman is immune. • You can make the diagnosis by observing that the vaginal pH is more alkaline than the usual 4.5. • And the bacteria cling to epithelial cells, creating the fuzzy-looking "clue cell" in pap smear. • Gardnerella is today's "usual suspect" for producing many cases of premature rupture of the membranes, premature labor, and premature birth.
Yeast infection • Vulva, vagina, cervix • red, itchy rash • visible fungal colonies visible. • Yeast infections are more likely when there is more glucose in the area • pregnancy, • oral contraceptive pill, diabetes), • when the normal bacteria are suppressed with antibiotics.
Trichomonas • Vulva, vagina, cervix • Trichomonas vulvovaginitis • a bad-smelling, red ("strawberry") inflammation with a thin discharge. • The protozoan is easily seen in wet mounts, looking like a bouncing pear moving about with flagella.
Ectopic breast tissue is fairly common on the vulva. It can enlarge during pregnancy and lactation. • Bartholin glands on either side of the vaginal introitus are prone to acute infection by ordinary bacteria, chlamydia, or gonorrhea. • Abscess formation may appear, • They can resolve, leaving the duct obstructed, and a cyst can form.
Skene's glands, on either side of the urethra, can also become inflamed, especially by gonorrhea. • Vestibular adenitis is a poorly-understood inflammatory process at the entry to the vagina. The glands are inflamed and very painful. They may be excised surgically for a cure.
Skin diseases including psoriasis, lichen planus, vitiligo, and familial pemphigoid, are very familiar on the vulva. • Vulvar hyperplasia: Sometimes the epidermis simply undergoes hyperplasia without anaplasia. It thickens ("acanthosis"), and becomes develops extra keratin ("hyperkeratosis").
Lichen sclerosus: ("chronic atrophic vulvitis") is a mysterious process in which a band of dense, homogeneous, hyaline collagen forms underneath the epidermis, which is thinned. The skin turns gray and parchment-like and becomes itchy. It can occur at any age. Although there is no anaplasia, a few percent turn malignant.
Papillary hidradenoma is an intraductal papilloma of the breast, only in the vulva along the embryonic milk like. • Mucosal polyps are skin tags, fibrous nodules covered with normal epithelium.
Condyloma acuminatum is the large, usually multiple warts that can occur on the vulva, perianal region, and (less often) the vagina and cervix. • HPV strains 6 and 11 as causes of condyloma acuminatum • Microscopically, a branching fibrous stalk with a thickened epithelium exhibiting these features of HPV infection: • hyperkeratosis • parakeratosis • koilocytes :cells with dark, wrinkled nuclei (from all those extra copies of the viral genome) • a perinuclear clear zone.
Vulvar intraepithelial neoplasia (VIN) • Epithelial dysplasia (macule, papule, plaque) • Atypia CIS • Etiology • HPV (16, 6, 11) • Histology: • VIN I, II, III (CIS).
3% of the Gyn cancers. • Exophytic (2/3), ulcerative, infiltrative. • Metastases: • ingiunal and femoral lymph nodes. • Most vulvar cancers are: • squamous cell carcinomas (most common), • adenocarcinomas, • melanomas, • basal cell carcinoma (less common).
Squamous cell carcinoma • Most squamous carcinomas are caused by HPV: • Preceded by dysplasia and carcinoma in situ ("vulvar intraepithelial neoplasia“; VIN), • which is analogous to the lesions in the cervix. • A physician may notice the premalignant lesions and excise them before cancer develops. • Squamous cell carcinomas not caused by HPV: • usually arise in lichen sclerosus or idiopathic hyperkeratosis. • These are more aggressive.
Extramammary Paget's disease • Mucin-rich cancer cells growing within the epidermis of the vulva or perineum • a red, itchy rash on Labium major. • Histology: • Tumor cells present clear cytoplasm which will stain for some sort of mucin (Paget cells). • Local excision should be curative. • The pathologist will do frozen sections to help see if the margins are free. • Even without excision, the lesion is likely to remain stable for a long time.
Paget’s disease: Cancer cells growing within the epidermis
DES bumps • Baby-girls exposed in utero to diethylstilbestrol (DES) often have glands in the upper vagina. • These appear as red bumps against the normally-pink mucosa. • These turn cancerous in fewer than 1% of affected girls. • Septate vagina • The only common non-iatrogenic birth defect is a septate vagina, from failure of the mullerian ducts to fuse. • There will also be a double uterus. • Gartner duct cyst • The only non-infectious, non-neoplastic lesion of the vagina • develops from the Wolffian duct remnants.
Squamous cell carcinoma • Disease of old age. • Caused by HPV. • Good prgonosis in Localized lesions.
Adenocarcinoma • Arises from the glands of girls exposed to DES, usually in their teens. • Only one in about 1000 of girls exposed in this way get cancer, • devastating. • The cells are glycogen-rich, hence the name "clear cell carcinoma".
Embryonal rhabdomyosarcoma • “Sarcoma botryoides", is a common malignant tumor of young children • Polypoid tumor (a bunch of grapes) • botryoidgrape-like. • The sarcoma contains cross-striated rhabdomyoblastic cells, • They are locally destructive and can metastasize late.