Download
1 / 54
540 likes | 683 Views
2011/12 Awareness and Early Diagnosis of Cancer Campaigns SHA Cluster Meetings October 2011. 1. Introduction: NAEDI Background. Improving outcomes for cancer patients: early diagnosis Cancer survival is a key measure of the effectiveness of healthcare systems.

E N D
2011/12 Awareness and Early Diagnosis of Cancer Campaigns SHA Cluster Meetings October 2011
1. Introduction: NAEDI Background • Improving outcomes for cancer patients: early diagnosis • Cancer survival is a key measure of the effectiveness of healthcare systems. • 1 year and 5 year survival rates are generally lower than comparable countries in Western Europe. • Coleman et al, Lancet 2010: Up to date survival trends show that improvements in cancer survival but the gap between countries remains. Differences are consistent with late diagnosis and differences in treatment. • NCIN Routes to diagnosis • Nearly 25% of newly diagnosed cancer patients came through as emergency presentations. • For all cancers (except acute leukaemia) 1-year relative survival rates were longer for patients presenting as emergencies than those presenting via other routes. • 10,000 deaths could be avoided each year in England if our cancer survival rates matched those in the best countries (e.g. Australia, Canada and Sweden).
1. Introduction: NAEDI Background • Policy Improving Outcomes: A Strategy for Cancer(Jan 2011) • Sets out the Government’s ambition to save an additional 5000 lives p.a. by 2014/15. This would bring survival in England up to the average for Europe. • £450 million over this Spending Review period to support work to improve earlier diagnosis. The Operating Framework for the NHS 2011/12 • Expects the NHS to implement IOSC and ensure patients have timely access to diagnosis and treatment.
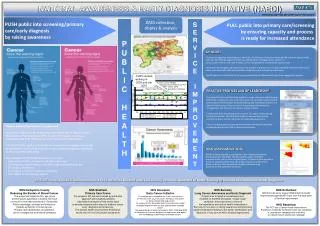
1. Introduction: NAEDI overview National Awareness and Early Diagnosis Initiative • 1. Raising public awareness of cancer symptoms and • encouraging earlier presentation • British public shows low awareness of symptoms of cancer and report barriers to seeing their GP. • Prioritising cancers by number of “avoidable deaths”. • Local testing → regional pilots → national campaigns. • Be Clear on Cancer campaigns from 2010/11. • Builds on local interventions since 2008.
1. Introduction: NAEDI overview National Awareness and Early Diagnosis Initiative • 2. Optimising clinical practice and systems • Aim is to drive earlier diagnosis in primary care in the • consultation setting, systems within the general practice or • system improvements between primary and secondary care. • Categories of intervention • Building GP Leadership capacity • Referral pathways and access to diagnostics • Continuing professional development • Awareness raising – preparing for patients • Organisational development • Audit • Clinical decision making • Network level activities • Approx £3 million to cancer networks in 2011/12
1. Introduction: NAEDI overview National Awareness and Early Diagnosis Initiative • 3. Improving access to diagnostics • Focus on: • Chest x-ray (lung cancer) • Lower GI endoscopy (bowel cancer) • Ultrasound (especially ovarian cancer) • MRI (brain tumours) • Guidelines for GPs: End of year • Baseline audit of Diagnostics (September 2010) • Diagnostic Imaging Dataset (In development)
1. Introduction: NAEDI overview National Awareness and Early Diagnosis Initiative • 4. Research, monitoring and evaluation • NAEDI research collaborative, coordinated by CRUK, to promote research on early diagnosis in areas including health services, awareness and presentation, methodology, screening, high risk populations. • R&D Policy Research Unit for Cancer Screening Awareness & Earlier Diagnosis. • International Cancer Benchmarking an international partnership coordinated by DH, NCAT and CRUK. • Health economics. • Monitoring and evaluation of early diagnosis interventions. • Monitoring progress against the level of ambition – 1 year survival rates in NHS Outcomes Framework.
1. Introduction: Overview of Campaigns 11/12 Overview of Public Awareness Campaigns 2011/12 • National campaign on bowel cancer symptoms – to launch 30 Jan 2012 for 9 weeks. • Regional campaign on lung cancer - Midlands and some bordering areas – launched 10 October 2011 for 5 weeks. • Local campaigns on oesophagogastric cancer, breast cancer in women over 70 and the symptom of blood in urine. 18 projects in 60+ PCTs from Jan – March 2012.
1. Introduction: Rationale for tumour sites Avoidable deaths pa if survival in England matched the best in Europe [NB Prostate has been excluded as survival ‘gap’ is likely to be due to differences in PSA testing rates.] Data derived from Abdel-Rahman et al, BJC Supplement December 2009c
2. NAEDI 2010/11 activity: Regional pilot NAEDI Regional Bowel Cancer Pilot 2010/11 • Campaign run in East of England and South West England for 7 weeks from end of Jan 2011. • Social marketing campaign using regional TV, radio and print media, face-to-face events and partnership activity.
2. NAEDI 2010/11 activity: Regional pilot Pilot results • Campaign recognition was high with 75% of the public both in South West and East of England claiming to have seen the advertising. • Very high levels of support for the campaign from the public (96%) and GPs (89%). • 48% increase in attendances in primary care of people over 50 with relevant symptoms – equates to 1 extra patient per week per practice. • 32% increase over a 6 month period in 2ww colorectal referrals during the campaign (up to 100% in some areas). • 28.5% increase in number of people waiting for a colonoscopy in East of England and 16.4% increase in South West England (some Trusts in core TV coverage in South West saw up to a doubling in colonoscopy waits). • There appears to be some effect on screening uptake and we are revisiting the data for both regions. • Complete data on number of patients diagnosed and stage at diagnosis due in October. • Final report to be published by the end of the year.
2. NAEDI 2010/11 activity: Regional pilot Pilot resultsUnprompted recall of symptoms in South West Source: TNS BMRB, pre/post tracking among general public Base: All respondents– Regional pilot : (SW Pre/Post: 475/510)
2. NAEDI 2010/11 activity: Regional pilot Pilot resultsUnprompted recall of symptoms in East of England Source TNS BMRB, pre/post tracking among general public Base: All respondents– Regional pilot : (EE Pre/Post: 490/475)
2. NAEDI 2010/11 activity: Regional pilot Pilot results: Attendances to primary care Source: Bowel Cancer Awareness Campaign Evaluation [Mayden, June 2011]
3. National Campaign on Bowel Cancer 2011/12 National Bowel Cancer Awareness Campaign 2011/12 • Campaign strategy • Objectives • Timing • Audience • Communication channels • Creatives • Key messages • Research • Campaign impact • Primary Care • Secondary Care
3. National Campaign on Bowel Cancer 2011/12 National Bowel Cancer Campaign Strategy • Objectives • Raise awareness of symptoms. • Encourage those with symptoms to visit GP, to increase presentations. • Increase numbers of cancers diagnosed at an earlier stage. • Timing • 9 week campaign to launch 30 Jan 2012.
3. National Campaign on Bowel Cancer 2011/12 National Bowel Cancer Campaign Strategy • Target audience: • 55+ C2DE as more likely to be diagnosed with cancer. • Communication channels: • TV; National press and women’s magazines; Radio; Out-of-Home; Events. • Key ethnic TV channels and press titles. • Online – paid-for search; display advertising and online content. • Commercial partnerships. • Non-commercial partnerships/support (public sector e.g. libraries, Citizens Advice Bureaux). • PR.
3. National Campaign on Bowel Cancer 2011/12 National Bowel Cancer Campaign Strategy • Creative Approach • Establish overarching proposition – Be Clear on Cancer – used as a brand stamp on the advertising. • “Originate once” approach results in economies of scale. • Ensure consistency of messaging. • The Doctor: both an advocate and an authority at the campaign’s heart. • Encourages people to tell their doctor if they recognise the signs and symptoms of cancer. • Our ambition is to create a positive campaign brand for the target audience to: • become clear about the symptoms of bowel cancer • the action they need to take (visiting their GP) • the benefits of doing so (cancer is treatable if caught early and the symptoms are often nothing to worry about).
3. National Campaign on Bowel Cancer 2011/12 National Bowel Cancer Campaign TV Advert The TV advert is hosted on the NHS Choices website. Click the link to watch the 30 second advert: http://www.nhs.uk/bowelcancer/Pages/bowel-cancer.aspx
3. National Campaign on Bowel Cancer 2011/12 National Bowel Cancer Campaign Strategy Key Messages • Original messages developed based on research and expert group advice. • Review of campaign messages in August 2011. • Lessons learned • Retain “3 weeks” symptom duration message but issue clearer advice to GPs that they are to exercise their own clinical judgement in referrals • Flexible use of some collateral e.g. targeting BME groups • Language appropriate – only 2 public complaints about the use of the word “poo”.
3. National Campaign on Bowel Cancer 2011/12 Evaluation: Measure campaign awareness Two phases of quantitative research: • Public, over 55s • Pre and post tracking surveys, face-to-face • In England • 1,100 interviews at both pre and post waves. • GP Survey • Pre and post tracking surveys, telephone • In England • 300 interviews at both pre and post waves. All conducted by TNS BMRB.
3. National Campaign on Bowel Cancer 2011/12 Bowel Campaign Evaluation Metrics
3. National Campaign on Bowel Cancer 2011/12 Implications for the NHS Primary Care (GPs, Practice Staff and Pharmacists) • Anticipate a manageable increase in attendance of patients with relevant symptoms - ~ increase of 1 extra patient per week per practice from start of campaign. • Estimate 50,000 nationwide. • Primary Care resources produced by Bowel Cancer UK. • Cancer Networks will be actively working with local GPs on the campaign plans and impact. • Planned letter from Prof Sir Mike Richards, National Cancer Director, to GPs informing them of the campaign. • Working with Professional Bodies to promote the campaign e.g. RCGP, MDU.
3. National Campaign on Bowel Cancer 2011/12 Implications for the NHS Secondary Care (Gastroenterologists, Coloproctologists, Histopathologists, NHS Managers) • Letter from Bruce Keogh, NHS Medical Director, in August informing the NHS about plans for the campaign. • Letter from Jane Allberry, Deputy Director for Cancer, in August, asking SHA Cancer Leads and Cancer Network Directors to start preparing for the campaign. • Increase in urgent GP referrals for suspected Lower GI; pilot showed a peak 4 weeks into the campaign, then a moderate decline but in some trusts referrals have not gone back to pre campaign levels. • Increase in colonoscopies: need to plan for short term as well as find longer term sustainable solutions. • Share more detailed modelling work on endoscopy demand and capacity. • Cancer Networks will be actively working with secondary care community to prepare for the campaign.
3. National Campaign on Bowel Cancer 2011/12 Cancer Network – Clinical Engagement (1) • Work with Cancer Network clinical leads – secondary care, GP, public health plus early diagnosis lead • Give clinicians the big picture. • Give precise information about exactly what is happening nationally and locally. • Spread the information as widely as possible. • Use clinicians to sign communications. • Communicate regularly without bombarding clinicians. • Share the results from the regional bowel pilot.
3. National Campaign on Bowel Cancer 2011/12 Cancer Network – Clinical Engagement (2) • Listen to and act on feedback. • Take time to discuss issues with clinicians. • Stress that GPs must use their clinical judgement in the consultation – the campaign is not telling them how to do their job. • More information • Guide to engaging GPs and primary care in the awareness and early diagnosis of cancer some tips based on presentations and discussions from a wide range of professionals involved in NAEDI at Sharing and Learning Sets organised by NCAT. (http://ncat.nhs.uk/sites/default/files/Guide to engaging GPs and primary care in the awareness and early diagnosis of cancer.doc )
3. National Campaign on Bowel Cancer 2011/12 Key messages on lower GI endoscopy • Lower GI endoscopy saves lives. • Lower GI endoscopy activity in England is very low in comparison with other countries (including Scotland). • Some Trusts still have unacceptable waiting times (>6 weeks), precluding full roll out of bowel cancer screening to people aged 70-75. • Activity is set to increase markedly over the next five years. Increased capacity needs to be planned for now. • A national awareness campaign on bowel cancer will create extra demand in early 2012: Plan now. • Lower GI endoscopy is highly cost effective. • Increased activity must not compromise quality and patient safety.
3. National Campaign on Bowel Cancer 2011/12 Key message 1: Lower GI endoscopy saves lives • Bowel cancer screening by FoBt and colonoscopy reduces mortality by around 16%. This should be available for all people aged 60-75 in England. • A UK trial has shown that a one-off flexible sigmoidoscopy reduces both incidence 23% and mortality 31%. This will be introduced across England over the next five years at age 55. An Italian trial has confirmed the UK findings. • Colonoscopy is a key diagnostic test for patients presenting symptomatically with bowel cancer.
3. National Campaign on Bowel Cancer 2011/12 Key message 2 : Activity in England is low • Colonoscopy rates (per 1000 population) England 8 Norway 10 Scotland 12 Poland 12 Australia 22 Alberta – Canada 21 Nova Scotia – Canada 26 • And…there are variations within England. Particularly low endoscopy rates are observed in the south of the country.
3. National Campaign on Bowel Cancer 2011/12 International comparisons - crude colonoscopy rates per 1,000 in 2010/11
3. National Campaign on Bowel Cancer 2011/12 Key message 3: Some Trusts have unacceptable waits • Colonoscopy and flexible sigmoidoscopy are a major cause of diagnostic waits exceeding 6 weeks. • The Cancer Reform Strategy committed the NHS to extend bowel cancer screening to men and women aged 70-75 from April 2010. • Only 33/58 screening centres have commenced this age extension (at October 2011). Long endoscopy waits are the main barrier to extending bowel cancer screening to age 70-75 in the remaining areas.
3. National Campaign on Bowel Cancer 2011/12 Key message 4: Activity is set to increase markedly • There are 5 key drivers of increased endoscopic activity: • Extension of FoBt screening to age 70-75 (underway). • Increases in symptomatic referrals requiring flexible sigmoidoscopy and/or colonoscopy – partly driven by awareness campaigns. • Flexible sigmoidoscopy screening (planned). • Increased surveillance activity (e.g. of patients found to have polyps). • Shift from barium enema to colonoscopy.
3. National Campaign on Bowel Cancer 2011/12 Expansion of the BCSP and commitments in the Cancer Outcome Strategy mean that there will be additional intensive pressures on endoscopic activity for the next 5 years Note: For the historical data the difference between the pink and blue lines largely reflects the current impact of bowel screening on endoscopy
3. National Campaign on Bowel Cancer 2011/12 Increase in lower GI endoscopic activity (rounded figures) The NHS needs to plan for a year on year increase of around 10% - 15% (i.e. around 120,000 more lower GI endoscopies each year)
3. National Campaign on Bowel Cancer 2011/12 Capacity/workforce implications • 45,000 additional colonoscopies a year (each year) = 9000 “sessions”. • 85,000 additional flexible sigmoidoscopies a year (each year) = 8500 “sessions”. • An average sized Trust will need 110 extra sessions pa (year on year) i.e. 2 sessions per week. • For a large Trust this will be 220 extra sessions pa (year on year) i.e. 4 sessions per week.
3. National Campaign on Bowel Cancer 2011/12 Key message 5: Plan for early 2012 now • Regional bowel cancer awareness pilots were undertaken in the East of England and the South West in January – March 2011. • 2ww colorectal referrals and lower GI endoscopy activity increased markedly – but just for the 9 week duration of the Campaign. • While the impact ranged across Trusts some observed up to a doubling of colonoscopy activity. • A national bowel cancer awareness campaign will be undertaken in January – March 2012. We estimate that this will generate around 15,000 additional colonoscopies nationally. • Trusts/commissioners need to plan now.
3. National Campaign on Bowel Cancer 2011/12 Impact of pilot campaign on colonoscopy activity and waiting list
3. National Campaign on Bowel Cancer 2011/12 Planning for early 2012 • 15000 additional colonoscopies across England equates to ... • Approximately 100 additional colonoscopies at an average sized NHS Trust (and 100 additional colonoscopies for an average sized PCT). • This will be spread over 8 to 10 weeks, so an average Trust will need to undertake around 10 additional colonoscopies (i.e. 2 sessions) per week for 10 weeks. For a large Trust this figure is likely to be doubled. • The total cost of 15,000 colonoscopies is around £9m. The cost to an average PCT or Trust is likely to be around £50,000. • Funding for this is in PCT baselines.
3. National Campaign on Bowel Cancer 2011/12 What activity levels in 2011/12 could look like - colonoscopy
3. National Campaign on Bowel Cancer 2011/12 What activity levels in 2011/12 could look like - flexi-sigmoidoscopy
3. National Campaign on Bowel Cancer 2011/12 Requirement to introduce additional endoscopy services Operating Framework for 2011/12 4.35 The NHS will be expected to implement the forthcoming Improving Outcomes Strategy for Cancer. Patients should have timely access to diagnosis and treatment and be seen by the right person with the appropriate expertise. In particular: • commissioners and local providers will want to consider the four priority areas for diagnostics for improving earlier diagnosis of cancer and ensure continuity of commissioning and provision is secured in the move to commissioning by the NHSCB and GP consortia: • chest x-ray: to support diagnosis of lung cancer; • non-obstetric ultrasound: to support diagnosis of ovarian cancer; • flexi sigmoidoscopy/colonoscopy: to support the diagnosis of colorectal cancer; and • MRI brain: to support diagnosis of brain cancer.
3. National Campaign on Bowel Cancer 2011/12 Details of funding from the Cancer Outcomes Strategy Impact Assessment The following sums have been allocated for promoting awareness and early diagnosis, including additional costs of diagnostic tests and treatment: • 2011/12 - £33m • 2012/13 - £136m • 2013/14 - £146.7m • 2014/15 - £198m This funding is going into PCT baselines – on the basis that the NHS will use the money to improve survival rate through earlier diagnosis i.e. it takes account of the additional tests needed.
3. National Campaign on Bowel Cancer 2011/12 SHA Breakdown of Colonoscopy procedures needed to meet underlying growth plus commitments in the cancer outcomes strategy – long term
3. National Campaign on Bowel Cancer 2011/12 SHA Breakdown of Flexisig procedures needed to meet underlying growth plus commitments in the cancer outcomes strategy – long term
3. National Campaign on Bowel Cancer 2011/12 Key message 6: Lower GI endoscopy is highly cost effective • Increased diagnostic activity will prevent cancer and lead to earlier diagnosis. • This will reduce the incidence of metastatic cancer (with associated costs). • Health economic modelling undertaken to inform development of the Cancer Outcomes strategy indicated a cost per year of life saved of £6241. • This suggests that earlier diagnosis would be very cost effective.
3. National Campaign on Bowel Cancer 2011/12 Costs of lower GI endoscopy
3. National Campaign on Bowel Cancer 2011/12 Key message 7: Increased activity must not compromise quality and patient safety • Previous work to improve quality through JAG. • No compromise in terms of quality of endoscopy services – working closely with National Clinical Director, British Society of Gastroenterologists and Association of Coloproctologists. • Further information to follow on this issue.
3. National Campaign on Bowel Cancer 2011/12 Summary: Lower GI endoscopy services • Action is needed now: • To prepare for the national awareness campaign in early 2012. • To deal with existing endoscopy waits to enable extension of screening to people aged 70-75 where necessary. • To prepare for the longer term need to expand endoscopy capacity. • Although there will be costs and workforce implications, this will save lives and will be highly cost effective.
2. NAEDI 2010/11 activity: Regional pilot Regional Lung Cancer Campaign Pilot • Regional pilot: • Test before commit to national roll-out. • Bowel cancer methodology - 2 regions – East & West Midlands (10 October – 13 November 2011). • Use BCOC creative look and feel. • Channels to include: • Regional TV; Press; Radio; Pharmacy bags; Screens in GP surgeries; Events. • No/low cost channels to include: • Commercial partnerships. • Non-commercial partnerships/support (public sector e.g. libraries, Citizens Advice Bureaux). • Media coverage - DH press office.
2. NAEDI 2010/11 activity: Regional pilot Lung Cancer Press Ad