Download
1 / 33
550 likes | 1.32k Views
-Explain the underlying mechanism of organogenesis as it relates to the development of the basic embryonic body plan. -Describe the development of the neural tube with respect to the process of neurulation , the function of the notochord, and the process of spinal cord development.

E N D
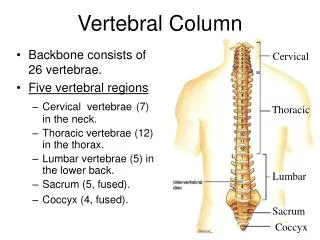
-Explain the underlying mechanism of organogenesis as it relates to the development of the basic embryonic body plan. -Describe the development of the neural tube with respect to the process of neurulation, the function of the notochord, and the process of spinal cord development. -Describe the normal development of the vertebral column with respect to cell line differentiation and structure formation. -Describe the common formation abnormalities that manifest clinically such as spina bifida and congenital scoliosis. Vertebral Column- 4th Week OnwardSept 29th, 2014 Christopher Ramnanan, Ph.D. cramnana@uottawa.ca
Rapid Growth in 3rd week is marked by: • Gastrulation: differentiation of the three germ layers (ectoderm, mesoderm, and endoderm) that will give rise to all embryonic tissues; the bilaminar embryonic disc becomes the trilaminar embryonic disc • Formation of the Primitive Streak: a thickened, linear band of epiblast that appears caudally in the median plane of the dorsal aspect of the trilaminar disc(the first morphological marker of gastrulation) • The Development of the Notochord: a solid cord of cells in midline that will underlie the neural tube and serve as the basis for the embryonic axial skeleton
Region of Prechordal Plate (deep to epiblast) Primitive node/knot: cell proliferation at cranial aspect of primitive streak; major molecular regulator of gastrulation The migration of primitive streak epiblastcells ventrally: invaginations forms endoderm and mesoderm; cells that do not migrate become ectoderm The migration of prenotochordal cells cranially: these cells will reach the prechordal plate (area just caudal to oropharyngeal membrane); these cells will first form the notochordal plate and then eventually form the definitive notochord Note: Prechordal plate cells are molecular regulators of forebrain and eye development
Peripheral Nervous System includes: Cranial Nerves (PNS nerves arise from brain, exit cranium) Spinal Nerves (PNS nerves arise from the spinal cord, exit vertebral column)
Paraxial Mesoderm (Somites)Dermatomes, Myotomes, and Sclerotomes(Vertebral Column) Ectoderm Neuroectoderm Neural Tube (CNS: Brain and Spinal Cord) + Neural Crest (Dorsal Root Ganglia, PNS Ganglia, Meninges)
Development of the Notochord Note: Cranial to Caudal Development Sagittal section 17 days: note cranial end of notochord proper has formed; caudally prenotochordal cells are still intercalated with endoderm to form notochordal plate; note location of prechordal plate caudal to oropharyngeal membrane Xsection ‘B’ 17 days: note notochordal plate in this area is attached/intercalated with endoderm Xsection ‘C’ 17 days: note notochordal plate in this area has detached from endoderm to form notochord
Notochord and Neurulation -Neurulation: Process by which neural plate forms the neural tube (primordial CNS development) - The developing notochord induces/signals the overlying ectoderm to thicken, forming the neural plate (first step in neurulation) -Neural plate = neural groove and neural folds -In addition to playing key role in initial CNS development (neurulation), notochord serves as basis for axial skeleton development (ex. vertebral bodies from somites)
Notochord and Neurulation (continued) Fig C: Fusion of neural folds begins in cervical region (5th somite level). Note the ‘zippering’ will continue until both cranial and caudal neuropores(openings) are closed (Days 25 and 28, respectively); these closures signify the completion of neurulation Fig D and E: Neural folds progressing to midline and fusing, forming neural tube. Note presence of neural crest cells bilaterally
Neural Crest Cells These neuroepithelial cells are at the border of the neural plate (neural folds). As the neural folds fuse progress/fuse in the midline, the neural crest cells dissociate from their neigbours and undergo epithelial-to-mesenchymal transformation and actively migrate to underlying mesoderm. Derivatives (shown): dorsal root ganglia, sympathetic and enteric ganglia, adrenal medulla cells Other derivatives (not shown) include: parasympathetic ganglia, meninges, melanocytes, craniofacial skeleton, Schwann cells, glial cells, and others (!)
FYI: View of Adult Posterior Body Wall Suprarenal Glands Preaortic (Sympathetic) Ganglia (associated with aorta) will supply abdominal viscera Sympathetic Trunk (Ganglia): paravertebral location
Somites 20 Days Somites: segmental (in cranial-caudal orientation) arrangement of paraxial mesoderm (adjacent to neural tube formation) Somites begin appearing at end of 3rd week, and all somites are apparent (42-44 pairs in humans) by end of 5th week
Neural tube Somite Ectoderm Developing somite Unsegmented paraxial mesoderm
Each somite will give rise to its own dermis (dermatome), skeletal muscle (myotome), and connective tissue (sclerotome, ie. bone, cartilage, tendon). Each dermatome and myotome retains its segmental innervation through development (regardless of where cells migrate).
Bones of the face and skull are derived from both neural crest and somite cells Fibrous joints b/w the bones of the neurocranium aren’t fully ossified until early childhood. The membranous gaps (fontanelles, or ‘soft spots’) facilitate brain enlargement in early life in both transverse and anterior-posterior planes. Clinical Correlate: Abnormally early fusion of the cranial sutures (craniosynostosis) can impair brain , skull, and and facial bone formation. Surgical disruption of prematurely closed sutures usually deemed necessary.
Cephalic End of Neural Tube3 Swellings Forebrain, Midbrain, and Hindbrain Note: Details for secondary vesicle formation, adult derivatives in Unit III
Clinical Correlate: Hydrocephalus Aberrant pooling of CSF in brain ventricles increases intracranial pressure, enlarging cranium (prior to fusing of cranial sutures) and will likely impair brain development. Treatment: Surgical shunting of fluid from ventricle space to peritoneal cavity. Hydrocephaly is common consequence of neural tube defects (NTDs) and usually involves herniation of part of the cerebellum into the foramen magnum (Arnold-Chiari malformation).
Development of the Spinal Cord (X-section) • The inner walls (neuroepithilium) of the neural tube thicken, forming 3 layers: • Ventricular Zone: gives rise to glioblasts and neuroblasts • Intermediate Zone (Mantle Layer): location of gray matter (cell bodies) • Marginal Zone: location of white matter of spinal cord (axons) Ventricular Zone Posterior Roots Intermediate Zone Marginal Zone Anterior Roots
Intermediate Zone Ventricular Zone Cells from the ventricular (neuroepithelial) zone proliferate and migrate to the intermediate (mantle) zone where they form two collections of cells (alar plates posteriorlyandbasal plates anteriorly ) separated by a groove (sulcanslimitans). Cells in the alar plate become the afferent (sensory) neurons of the dorsal horn. Cells in the basal plate become the efferent (motor) neurons of the ventral horn. The ventral horns grow/bulge, forming the ventral median fissure. The dorsal horns merge, forming the dorsal median septum. The lumen of the neural tube narrows and becomes the central canal. The marginal layer gives rise to the white matter of the spinal cord.
Development of the Spinal Cord (Cranial-Caudal) A In the third month development, spinal cord extends length of the embryo; spinal nerves pass through IV foramina at level of origin B-C The length of embryo, vertebral column, and dural sac lengthen more rapidly than spinal cord D At maturity, spinal cord ends at ~L2 (medullary cone). Dural sac and subarachnoid space extend to S2. Clinically: If spinal cord is tethered distally, lower spinal cord functions (motor+sensory to lower back, lower limb, urinary and bowel function) can be impaired
Development of the Vertebral Body Condensation of sclerotome cells around neural tube posteriorly (neural arch) and anteriorly (centrum) Neural Arch Vertebral Arch Centrum Vertebral Body Primary ossification centers bilaterally in neural arch and in centrum
Vertebral Body: 1ovs 2o Ossification Centers Primary ossification centers evolve in the centrum and the neural arch (7-8 weeks in development). Secondary ossification centers evolve in the spinous process, transverse processes, and anular epiphysis (puberty).
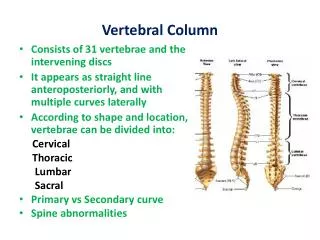
Development of the Vertebral Column Note: Sclerotome condenses to form vertebral bodies following segmental arrangement of somites; notochord disintegrates at these levels and only persists as the nucleus pulposus in each IV disc
Clinical Correlate: Hemivertebrae Bilateral nature of centrum formation and arch formation results in potential for partially formed (deformed) vertebra: Hemivertebrae. These malformations can alter shape and/or number of vertebrae, potentially resulting in -Scoliosis, Lordosis, or Kyphosis -aberrant formation of IV foramina (and impingement of nerves)
Clinical Correlate: Persistent Notochord Failure of notochord to obliterate may cause back pain but is typically asympomatic. Associated with ‘Butterfly vertebrae’ (cleft through a body corresponding to persisting notochord). Severe ‘butterflying’ can cause instability of vertebral column. Figure from Cotton et al., Neuroradiology (1995) 37: 308-310
Clinical Correlate: Klippel-Feil Syndrome Abnormal segmentation of cervical somites can lead to inappropriate fusion of adjacent cervical vertebra (can involve anywhere b/w 2 vertebrae and the entire C-spine). Most commonly involves fusion of C2 and C3 (shown here). Cardinal characteristics include: -Short neck -Limited cervical mobility -Low hairline
Neural Tube Defects (NTDs) Most NTDs of the spinal cord result from abnormal closure of the neural tubes in week 4 of development. NTDs include abnormal development of the neural arches (spina bifida). These neural tube defects may involve multiple layers of spinal cord protection (meninges, vertebrae, muscles, skin) and can be caused by genetic, environmental, and nutritional factors (ex. valproic acid, folate deficiency). Most cases involve the L5-S2 region.
Spina bifida occulta: small defect in neural arch such that spinal cord unable to herniate posteriorly. Neural tissue typically unaffected. Overlying skin sometimes marked by dimples and/or small tuft of hair. Least severe form of spina bifida, typically asymptomatic. Tethered cord syndrome may present in unique circumstances. http://www.spinabifidaassociation.org/site/c.evKRI7OXIoJ8H/b.8277207/k.6DCB/Spinal_Cord_Tethering.htm B. Meningocele: neural arch defect allows for meninges/subarachnoid space to protrude posteriorly (neural tissue does not herniate). C. Meningomyelocele: Defect in which meninges and neural tissue both protrude posteriorly. Myeloschisis (shown on next slide): Defect in which neural tissue is open to outside world (no overlying membrane). Spinal cord in affected region presents as flat mass of neural tissue. Most severe form of spina bifida.
More severe forms of spina bifida (B-D) call for surgical intervention in first few days of life. Surgeries have been performed as early as 22 weeks in utero. Review: Anesthesiology. 2013 May;118(5):1016-8. Complications tend to increase with the types of spina bifida with greater neural tissue risk (C, D) and when the spina bifida defect occurs more cranially. Meningomyelocele and myeloschisis are associated with increased risks for infection, problems with lower limb function, and loss of muscle tone. .
B C A Note: Spina Bifida w/Myeloschisis can be berefered to Spina Bifida Aperta (“open”) Spina Bifida w/Meningocele or w/ Meningomyelocele can be referred to as Spina Bifida Cystica (‘cyst’ like appearance) A Spina Bifida Occulta B Spina Bifida Meningomyelocele C Spina Bifida Myeloschisis
Failure of cranial neuropore to properly close can cause: Anencephaly -failure to form major parts of brain, scalp, face (typically only brainstem is formed) Encephalocele -variations where structures (meninges, brain, ventricle) space can herniate through posterior skull Meningoencephalocele Meningocele Meningohydroencephalocele http://www.ninds.nih.gov/disorders/cephalic_disorders/detail_cephalic_disorders.htm
Organogenesis -The process by which each of the ectoderm, mesoderm, and endoderm will give rise to all specific tissues and organs of the body -Organogenesis occurs during the embryonic period (3rd to 8th weeks of development). -The extensive proliferation/growth of the CNSand other organ systems cause the flat embryonic disc to fold upon itselfin lateral and cranio-caudal planes. This folding, in turn, play a role in regulating normal organogenesis and morphology. http://www.youtube.com/watch?v=BaafWRqdjLw