Download
1 / 133
1.34k likes | 1.54k Views
Periodontics. Dentalelle Tutoring. The Periodontium.

E N D
Periodontics Dentalelle Tutoring
The Periodontium AB, alveolar bone; AC, alveolatrcrest; AM, alveolar mucosa; AP, alveolar process; CB, compact bone of alveolar bone proper; CEJ, cemento-enamel junction; CT, connective tissue; DEJ, dentino-enamel junction; ES,enamel space; G, gingiva; GE, gingival epithelium; GG, gingival groove; GM, gingival margin; GS, gingival sulcus; JE, junctional epithelium; MGJ, mucogingival junction; MS, marrow space; OE, oral epithelium; PDL, periodontal ligament; RCE, radicular (root) cementum; SE, sulcular epithelium;
Incisor AB, alveolar bone; C, incisive canal; CE, cementum; F, foramen; G, gingiva; MGJ, mucogingival junction; PDL, periodontal ligament
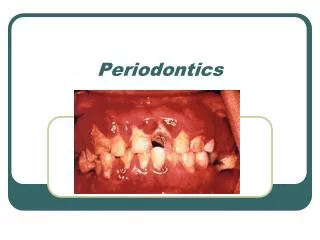
Periodontium • Composed of: • Gingiva • Cementum • Alveolar Bone • Periodontal Ligament
Gingiva • The gingiva is the keratinized mucosa that surrounds the teeth. It forms a collar around each tooth, that ranges in width from 1 to 9 mm. The narrowest zone of the gingiva is usually found on the buccal surface of the mandibular canine to first premolar region. • The widest zone is often located on the lingual aspect of the last mandibular molar. The gingiva is attached in part to the cementum of the tooth and in part to the alveolar process. The gingiva is composed of masticatory mucosa.
Features • In light-skinned individuals the gingiva can be readily distinguished from the adjacent dark red alveolar mucosa by its lighter pink color. Its apical border, that separates it from the adjacent alveolar mucosa, is the mucogingival junction. A similar tissue relationship can be seen on the lingual aspect of the mandible. • In dark-skinned persons the gingiva may containmelanin pigment to a greater extent than the adjacent alveolar mucosa. The melanin pigment is synthesized in specialized cells, the melanocytes, located in the basal layer of the epithelium. The melanin is produced as granules, themelanosomes, that are stored within the cytoplasm of the melanocytes, as well as the cytoplasm of adjacent keratinocytes. Melanocytes are embryologically derived from neural crest cells that eventually migrate into the epithelium. If pigmented gingiva is surgically resected, it will often heal with little or no pigmentation. Therefore, surgical procedures should be designed so as to preserve the pigmented tissues.
The Gingiva • The mostcoronal portion of the gingiva is the gingival margin. The term marginal gingiva refers to that portion of the gingiva that is located close to the gingival margin. • The gingival sulcus is the shallow groove between the marginal gingiva and the tooth. • The gingival groove is an indentation that parallels the oral or vestibular surface of the gingival margin. It is located at about the same level as the apical border of the junctional epithelium. Note: its level does not correspond to that of the bottom of the gingival sulcus. It is only present occasionally. Its presence or absence is not related to gingival health. Inflammation may cause the tissues to swell and mask its presence.
Free and Attached • Clinicians sometime use the terms "free" and "attached" gingiva. Although these terms may have some clinical relevance, they are anatomically incorrect. The determination as to whether the gingiva is "free" or "attached" is made by probing the gingival sulcus with a periodontal probe. • This instrument will frequently penetrate the junctional epithelium beyond the sulcus bottom, particularly in the presence of inflammation. This results in the clinical impression that the marginal gingiva is detached from the tooth to a much greater degree than is the case. Anatomically. "Attached" gingiva refers to the portion of the gingiva apical to the "free" gingiva which is firmly bound to the underlying tooth and alveolar process.
Interdental • The gingiva that occupies the interdental spaces coronal to the alveolar crest is the interdental gingiva. It is composed of a pyramidal interdental papilla in the incisor region. • In the posterior region it is composed of an oral and a vestibular papilla (P) joined by an interdental "col" (C). The interdental gingiva is attached to the tooth by junctional epithelium (JE) coronally and by connective tissue fibers apically (not shown). The most coronal portion of the interdental gingiva is lined with sulcular epithelium (SE)
Oral Epithelium • It is the stratified, squamous keratinizing epithelium, that lines the vestibular and oral surfaces of the gingiva. It extends from the mucogingival junction to the gingival margin, except for the palatal surface where it blends with the palatal epithelium. • The oral epithelium consists of a basal layer (stratum basale, SB), a spinous layer (stratum spinosum, SS), a granular layer (stratum granulosum, SG) and a cornified layer (stratum corneum, SC). It is designed primarily for protection against mechanical injury during mastication. • Resistance to mechanical injury is mediated primarily by the numerous intercellular junctions, mostly desmosomes, that hold the cells tightly together and the cornified layer. The cornified layer and the relatively narrow intercellular spaces also contribute to the relative lack of permeability.
The oral epithelium is connected to the underlying connective tissue of thelamina propria by an irregular interface. This interface consists of finger-like projections of connective tissue from the papillary layer extending into depressions on the undersurface of the epithelium. These depressions are located between the interconnected Rete ridges that form the undersurface of the epithelium. Cross-sections of these ridges, as seen in histological sections are sometimes referred to as Rete pegs. • Transmission electron micrograph of the junction between a basal cell of the gingival oral epithelium and the connective tissue of the underlying lamina propria. The epithelial cell (EC) contains widely dispersed cytoplasmic filaments, also known as tonofilaments. • The epithelial cell membrane facing the lamina propria is studded with numerous hemidesmosomes (HD) and is connected to it by a basal lamina(BL). The basal lamina consists of an electron-dense layer, the lamina densa (LD) and an electron-lucent layer, the lamina lucida (LL). The lamina densa is composed of an afibrillar type of collagen, type IV collagen. The lamina lucida is composed of laminin and other glycoproteins. Anchoring fibrils (AF), composed of type VII collagen, extend from the undersurface of the lamina densa into the lamina propria.
Sulcular Epithelium • It is the stratified, squamous epithelium, non-keratinized or para keratinized, that is continuous with the oral epithelium and lines the lateral surface of the sulcus. Apically, it overlaps the coronal border of the junctional epithelium, a structural design that minimizes ulceration of the epithelial lining in this region. This epithelium shares many of the characteristics of the oral epithelium (Fig. 10), including good resistance to mechanical forces and relative impermeability to fluid and cells.The overall structure of the sulcular epithelium resembles that of the oral epithelium, except for the surface layer that is less keratinized than its counterpart in the oral epithelium. This incomplete type of keratinization is referred to as parakeratinization. CT, gingival connective tissue; GS, gingival sulcus; PKE, parakeratinized epithelial layer.
Junctional Epithelium • It is the stratified non-keratinizing epithelium, that surrounds the tooth like a collar with a cross-section resembling a thin wedge. It is attached by one broad surface to the tooth and by the other to the gingival connective tissue. The junctional epithelium has 2 basal laminas, one that faces the tooth (internal basal lamina) and one that faces the connective tissue (external basal lamina). The proliferative cell layer responsible for most cell divisions is located in contact with the connective tissue, i.e. next to the external basal lamina. • The desquamative (shedding) surface of the junctional epithelium is located at its coronal end, which also forms the bottom of the gingival sulcus. • The junctional epithelium is more permeable than the oral or sulcular epithelium. It serves as the preferential route for the passage of bacterial products from the sulcus into the connective tissue and for fluid and cells from the connective tissue into the sulcus. • The term epithelial attachment: refers to the attachment apparatus, i.e. the internal basal lamina and hemidesmosomes, that connects the junctional epithelium to the tooth surface. This term is not synonymous with junctional epithelium which refers to the entire epithelium.
Segment of junctional epithelium (JE) from an area just apical to the gingival sulcus. The width of the junctional epithelium may consist of as many as 30 cells in the sulcus region to as few as one cell in its most apical portion. The intercellular spaces between the cells of the junctional epithelium are wider than in the oral or sulcular epithelia. This is due in part to the lower density of intercellular junctions between the cells of the junctional epithelium. The density of junctions is approximately one third of that in the oral and sulcular epithelium. • This section is unusual by the absence of inflammatory cells in the connective tissue adjacent to the epithelium. • Transmission electronmicrograph of normal, uninflamed junctional epithelium (JE). The cells are orientated with their long axis parallel to the tooth surface. The intercellular spaces are relatively narrow. The epithelium is attached to the enamel by an internal basal lamina (IBL) and to the connective tissue (CT) by the external basal lamina (EBL). ES, enamel space. • The cytoplasm of the junctional epithelium contain dispersed tonofilaments, but lack tonofibrils. Under normal circumstances these cells do not undergo keratinization.
Transmission electronmicrograph of junctional epithelium in inflamed gingiva. Note the marked distension of the intercellular spaces by polymorphonuclear leucocytes (PMN) that are migrating from the connective tissue toward the gingival sulcus (located toward the top of the micrograph). Fluid exudate from the connective tissue also flows into the sulcus through the enlarged intercellular spaces. The spaces enlarge in part through rupture of the desmosomal junctions and in part because they become distended by inflammatory cells and fluid. • The bi-directional arrows indicate that the junctional epithelium (JE) is the most permeable portion of the gingival epithelia. Soluble substances can diffuse from the oral cavity into the underlying gingival connective tissue (CT), while both fluids and cells can travel through the junctional epithelium from the connective tissue into the gingival sulcus (S) on their way to the oral cavity. • Because of its permeability to bacterial products and other assorted antigens originating in the oral cavity, the connective tissue adjacent to the junctional epithelium tends to become infiltrated with chronic inflammatory cells, primarily lymphocytes and plasma cells. OE, oral epithelium; SE, sulcular epithelium.
Gingival Connective Tissue • The gingival connective tissue is composed of gingival fibers, ground substance, and cells, including neural and vascular elements. The bulk of the gingival connective tissue is composed of a dense, predominantly collagenous matrix that contains collagen fibers running in recognized fiber groups. These are referred to as the principal fibers of the gingival connective tissue. The dense gingival connective tissue is referred to as a lamina propria. It consists of the papillary layer, finger-like projections of connective tissue that are contained within depressions on the undersurface of the overlying epithelium, and the reticular layer, located between the epithelial undersurface and the root surface or adjacent alveolar process. • At its junction with the lining mucosa, in the region delineated by the mucogingival junction, the lamina propria becomes continuous with the much looser and elastic connective tissue of the alveolar submucosa.
The major components of the gingival connective tissue include the fibers, the ground substance or intercellular matrix, assorted cells, blood and lymphatic vessels, and nerves. The ground substance occupies the space between cells, fibers and neurovascular elements. • Its major constituents are water, glycoproteins and proteoglycans. The ground substance permits the diffusion of biological substances between various structural elements.
Gingival Fibers • Most of the fibers are composed of collagen, with minor contributions from elastic fibers and oxytalan fibers. • Elastic and oxytalan fibers are generally confined to perivascular regions, although oxytalan fibers are also found as thin fiber bundles within collagen-rich regions like the lamina propria.
Gingival Fibers - Collagen • Transmission electron micrograph of gingival connective tissue showing the intercellular junctions (ICJ) between cytoplasmic strands from adjacentfibroblasts. The fibroblasts form an interconnected network of cells, the intercellular spaces of which are filled with fibers and ground substance, the jelly-like material in which the fibers are embedded. The fibroblasts are responsible for the production of the fibers and ground substance. They are also capable of removing fibers and ground substance during remodeling of the gingival tissues. • Most of the fibers in gingival connective tissue are composed of collagen. The bulk of the collagen is type I collagen, the most abundant form of collagen in the human body. The structural unit of type I collagen is a typically striated fibril with a characteristic banding pattern that repeats every 64 nm. The banding results from the packing arrangement of the collagen molecules that make up the individual fibril
Fibrils • Type I collagen fibrils are normally organized into bundles of fibrils, or fibers. They are found throughout the lamina propria. • Type III collagen fibers are thinner than the type I fibers and tend to be found close to basal laminas of vascular channels and epithelial tissues. They stain readily with silver stains and probably account for most of the argyrophilic (silver stained) fibers seen in silver-stained sections. • They are also known as reticular fibers.
Gingival Fibers - Other • Type VII collagen is found as anchoring fibrils, located in intimate contact with epithelial basal laminas. In addition to the fibrillar forms of collagen mentioned above, type IV collagen, an amorphous form of collagen, is found in the basal laminas of the epithelial lining and blood vessel walls, primarily in the lamina densa. • The other fiber types found in the periodontium are elastic fibers and oxytalan fibers. Elastic fibers are rather scarce in the lamina propria. They are a more common constituent of the lining submucosa. They consist of 2 major components, microfibrils made of fibrillin and the amorphous component elastin. The latter provides the fiber with its elastic properties.
Note that elastic fibers consist of 2 distinct structural entities, a microfibrillar component (MF) composed of the proteinfibrillin, and an amorphous component (AE) that is composed of elastin, the protein that gives the fibers their elastic properties. As elastic fibers mature, the ratio of elastin to fibrillin increases. In the gingiva, most elastic fibers are immature and poorly developed.Oxytalan fibers are a fiber type related to elastic fibers. They appear to consist of the microfibrillar component only, thereby resembling very immature elastic fibers.
Fiber Groups • These are largely composed of collagenous fibers. The dentogingival fibers (A) insert into the supracrestal root cementum and fan out into the adjacent connective tissue. Thedentoperiosteal fibers (B) insert into the supracrestal root cementum and blend with the periosteal covering of the adjacent alveolar process. The alveologingival fibers (C) insert into the alveolar crest and fan out into the adjacent gingival connective tissue. Thecircumferential fibers (D) follow a circular course around individual dental units. • Thesemicircularfibers (E) insert on the approximal surfaces of a tooth and follow a semicircular course to insert on the opposite side of the same tooth. The transgingival fibers (F) insert into the approximal surface of a tooth and fan out toward the oral or vestibular surface. Theintergingival(G) fibers course along the oral or vestibular surfaces of the dental arch. Thetransseptalfibers (H) course from one approximal tooth surface to the approximal surface of the adjacent tooth.
Gingival Cells • The major cellular elements in the gingival connective tissue include: • Fibroblasts, macrophages, mast cells, osteoblasts and osteoblast precursor cells, cementoblasts and cementoblast precursor cells, osteoclasts and odontoclasts, assorted inflammatory cells, and cells that make up vascular channels and nerves. Inflammatory cells include polymorphonuclear leucocytes, lymphocytes and plasma cells. • Under normal circumstances they may be found in small numbers, as isolated cells. In the presence of inflammation they can be found in large numbers, often as dense cellular aggregates that have replaced the fibrous elements in the connective tissue. The connective tissue also contains undifferentiated ectomesenchymal cells that serve as a replacement source for more differentiated cells, primarily fibroblasts.
Fibroblasts are irregularly shaped cells responsible for the synthesis of various connective tissue fibers and the ground substance in which they are imbedded. They are also responsible for the removal of these structural elements. Therefore these cells play a key role in the maintenance and remodeling of the connective tissue.
Vessels and Nerves • (i) Blood supply: • The gingival blood supply originates from blood vessels in the periodontal ligament, the marrow spaces of the alveolar process and supraperiosteal blood vessels. These vessels in turn supply major capillary plexuses that are located in the connective tissue adjacent to the oral epithelium and the junctional epithelium. • (ii) Lymphatics: • The gingival tissues are supplied with lymphatic vessels that drain principally to submaxillary lymph nodes. • (iii) Nerves: • Branches of the trigeminal nerve provide sensory and proprioceptive functions. In addition, autonomic nerve endings are associated with the vasculature.
Connective Tissue – Epithelial Interactions • The interaction of connective tissues and adjacent epithelia have a significant effect on epithelial tissue differentiation. The dense lamina propria found under the masticatory mucosa is largely responsible for the maintenance of the stratified squamous keratinizing epithelium that covers it. Likewise, the loose connective tissue that supports the non-keratinizing lining epithelium is largely responsible for the absence of keratinization in this epithelium. • If a tissue graft consisting of lamina propria is taken from the masticatory mucosa of the hard palate and is transplanted to a region lacking an adequate covering of keratinizing mucosa, it will induce the epithelium that grows over it to keratinize, even if the epithelium originates from an adjacent, non-keratinized mucosal surface. • This property of the connective tissue to modulate the differentiation of the overlying epithelium is taken advantage of in reconstructive surgical procedures. For example, a palatal connective tissue graft can be transplanted subepithelially to a zone lacking keratinized mucosa, where it will induce the overlying epithelium to differentiate into a keratinized epithelium.
Supportive • The periodontal ligament serves primarily a supportive function by attaching the tooth to the surrounding alveolar bone proper. This function is mediated primarily by the principal fibers of the periodontal ligament that form a strong fibrous union between the root cementum and the bone. The periodontal ligament also serves as a shock-absorber by mechanisms that provide resistance to light as well as heavy forces. • Light forces are cushioned by intravascular fluid that is forced out of the blood vessels. Moderate forces are also absorbed by extravascular tissue fluid that is forced out of the periodontal ligament space into the adjacent marrow spaces. The heavier forces are taken up by the principal fibers.
Remodeling • The periodontal ligament also serves a major remodeling function by providing cells that are able to form as well as resorb all the tissues that make up the attachment apparatus, i.e. bone, cementum and the periodontal ligament • Undifferentiated ectomesenchymal cells, located around blood vessels, can differentiate into the specialized cells that form bone (osteoblasts), cementum (cementoblasts), and connective tissue fibers (fibroblasts). Bone- and tooth-resorbing cells (osteoclasts and odontoclasts) are generally multinucleated cells derived from blood-borne macrophages.
Sensory and Nutritive • The periodontal ligament also serves a sensory function. The myelinated dental nerves that perforate the fundus of the alveoli rapidly lose their myelinated sheath as they branch to supply both the pulp and periodontal ligament. The periodontal ligament is richly supplied with nerve endings that are primarily receptors for pain and pressure. • Finally, the periodontal ligament provides a nutritive function that maintains the vitality of its various cells. The ligament is well-vascularized, with the major blood supply originating from the dental arteries that enter the ligament through the fundus of the alveoli. Major anastomoses exist between blood vessels in the adjacent marrow spaces and the gingiva.
Cementum • Cementum may be found both on the root as well as the crowns of teeth. It may also vary in its structure. Some forms of cementum may be cellular, while others are not. Some have a fibrillar collagenous matrix, while others do not. • Cementum may be classified in the following ways: Radicular cementum: The cementum that is found on the root surface.Coronal cementum: The cementum that forms on the enamel covering the crown. Cellular cementum: Cementum containing cementocytes in lacunae within the cementum matrix. Acellular cementum: Cementum without any cells in its matrix. Fibrillar cementum: Cementum with a matrix that contains well-defined fibrils of type I collagen. Afibrillar cementum: Cementum that has a matrix devoid of detectable type I collagen fibrils. Instead, the matrix tends to have a fine, granular consistency.
Extrinsic fibercementum: Cementum that contains primarily extrinsic fibers, i.e. Sharpey's fibers that are continuous with the principal fibers of the periodontal ligament. Since the fibers were originally produced by periodontal ligament fibroblasts, they are considered "extrinsic" to the cementum. These fibers are orientated more or less perpendicularly to the cementum surface and play a major role in tooth anchorage. • Intrinsic fiber cementum: Cementum that contains primarily intrinsic fibers, i.e. fibers produced by cementoblasts and that are orientated more or less parallel to the cementum surface. This form of cementum is located predominantly at sites undergoing repair, following surface resorption. It plays no role in tooth anchorage. • Mixed fiber cementum: Cementum that contains a mixture of extrinsic and intrinsic fiber cementum.
Types • 1. Acellular, afibrillar cementum • This cementum is mostly composed of mineralized matrix, without detectable collagen fibrils or cementocytes. It is produced exclusively by cementoblasts. It is typically found as coronal cementum on human teeth. • 2. Acellular, extrinsic fiber cementum • This type of cementum has a matrix of well-defined, type I collagen fibrils. The fibrils are part of the, densely packed Sharpey's fibers, that are continuous with the principal fibers of the periodontal ligament. Because of their dense packing, the individual Sharpey's fibers that form the bulk of the matrix may no longer be identifiable as individual fibers within the cementum layer. This cementum, which is acellular, is located in the cervical two-thirds of the root of human teeth. It plays a major role in tooth anchorage.
3. Cellular, intrinsic fiber cementum • This cementum contains cementocytes in a matrix composed almost exclusively of intrinsic fiber cementum. It is located almost exclusively at sites of cementum repair. It plays no part in tooth anchorage. However, it may be covered over by extrinsic or mixed fiber cementum, both of which are able to provide new anchorage. • 4. Cellular, mixed fiber cementum • It is found on the apical third of the root and in furcations (i.e. between roots). In these locations, the rate of cementum formation is usually more rapid than in the cervical region. The mineralized, extrinsic collagen fibers (Sharpey's fibers) run a more irregular course than in acellular, extrinsic fiber cementum. Intrinsic fibers are found interspersed among the extrinsic fibers of the cementum matrix, so that individual Sharpey’s fibers are more readily identifiable than in extrinsic fiber cementum. Cementoblasts are trapped in hollow chambers (or lacunae) where they become cementocytes. • The thickness of radicular cementum increases with age. It is thicker apically than cervically. Thickness may range from 0.05 to 0.6 mm.
General • The alveolar process is the portion of the jawbone that contains the teeth and the alveoli in which they are suspended. The alveolar process rests on basal bone. Proper development of the alveolar process is dependent on tooth eruption and its maintenance on tooth retention. When teeth fail to develop (e.g. anodontia), the alveolar process fails to form. When all teeth are extracted, most of the alveolar process becomes involuted, leaving basal bone as the major constituent of the jawbone. The remaining jawbone, therefore, is much reduced in height. • The alveolar process is composed of an outer and inner cortical plate of compact bone that enclose the spongiosa, a compartment composed of spongy bone ( also called trabecular or cancellous bone). • It is important to distinguish between the terms "alveolar process" and "alveolar bone" .
Alveolar Bone/Alveolar Process • The alveolar bone proper lines the alveolus (or tooth housing) which is contained within the alveolar process. It is composed of a thin plate of cortical bone with numerous perforations ( or cribriform plate) that allow the passage of blood vessels between the bone marrow spaces and the periodontal ligament. • The coronal rim of the alveolar bone forms the alveolar crest, which generally parallels the cemento-enamel junction at a distance of 1-2 mm apical to it
Fenestration • Where roots are prominent and the overlying bone very thin, the bone may actually resorb locally, creating a window in the bone through which the root can be seen. This window-like defect in the bone is referred to as a fenestration (F)
Dehiscence • In some cases, as shown in this figure, the rim of bone between the fenestration and the alveolar crest may disappear altogether and produce a defect known as a dehiscence (D). Awareness of these defects is important when surgical flaps are reflected, as the exposure of such defects during surgery may aggravate their severity.
Bone Formation • Bone is produced by osteoblasts (OB) that are found in the periosteum, endosteum and periodontal ligament adjacent to bone-forming surfaces. These specialized cells originate from less differentiated precursor cells close to the bone. These cells are in turn derived from undifferentiated ectomesenchymal cells found in the periosteum, endosteum and the periodontal ligament. • During bone formation, osteoblasts become incorporated into bone as osteocytes (OC) that are completely surrounded by bone. The chamber in which they are trapped is called a lacuna (plur. lacunae). Osteocytes remain connected to osteoblasts and other osteocytes by cytoplasmic processes that run through small canals in the bone, or canaliculi (C).
Osteon • Cortical plate of compact bone in the mandible. The mandible is enveloped by a well-developed cortex of compact bone. The bulk of the compact bone consists of cylindrical units of bone, the osteons or Haversian systems (HS). • Each osteon has a central canal, the Haversian canal that houses a blood vessel. Haversian canals are linked to one another and the periphery of the cortex by Volkman canals that course perpendicularly to the Haversian canals. The outer and inner layers of the cortex consist of parallel lamellae of compact bone, called the external (ECL) and internal circumferential lamellae. The bone that fills the spaces between adjacent osteons is the interstitial bone.