Download
1 / 27
270 likes | 684 Views
New Concepts and Advances (Arthroscopic) for the Treatment of Shoulder Pain. William F Bennett MD. The Simple Shoulder. While a complex joint with complex function, general approaches to determining the non-descript, cause….is easy! I.e., intrinsic versus extrinsic. Intrinsic versus Extrinsic.

E N D
New Concepts and Advances (Arthroscopic) for the Treatment of Shoulder Pain William F Bennett MD
The Simple Shoulder • While a complex joint with complex function, general approaches to determining the non-descript, cause….is easy! • I.e., intrinsic versus extrinsic
Intrinsic versus Extrinsic • Intrinsic- later and more descript…means pain coming from the shoulder joint itself • Extrinsic- pain that may cause shoulder pain but comes from sources outside the shoulder
Extrinsic • Most common- cervical spine • Pancoast tumors of the lung • Thoracic spine • Peritoneal/Splenic irritation can cause pain at Erb’s point • Angina/MI • Metabolic/Oncologic problems, ie., bone marrow involvement like lymphoma/leukemia, parathyroid
Extrinsic-Cervical Spine • General rule--trapezial pain-cervical -deltoid pain- intrinsic or from the shoulder Can have both shoulder and cervical spine affected which makes it more difficult Cervical spine may have radicular involvement
Intrinsic • Once extrinsic has been ruled out then one can focus on the intrinsic causes. • If a certain shoulder motion whether it be flexion, abduction, external rotation or internal rotation causes pain in the deltoid area and not in the trapezial area, one is probably dealing with an intrinsic problem
Before discussing intrinsic Causes Lets diverge and discuss the anatomy and function of the shoulder
Anatomy • 4 joints-two are articulations • Glenohumeral joint • Acromioclavicular joint • Scapulothoracic articulation • Sternocalvicular articulation/joint • Discuss Bones-Bone models
Ligaments/Capsule • Capsule is the “sac” • Normal sac allows motion in various planes • Abnormal sac restricts motion in various planes • Ligaments- hold bone to bone • Glenohumeral ligaments • Coracohumeral ligaments • Coracoacromial ligaments • Coracoclavicular ligaments
Muscles/Tendons • Rotator Cuff are a confluence of 4 tendons from the following respective muscle bellies • Supraspinatus • Subscapularis • Infraspinatus • Teres minor • Biceps • Deltoid Bone models
Bursae/Cartilage/Meniscus • Subacromial Bursae • Subdeltoid bursae • Subcoracoid bursae • Glenohumeral articular cartilage • Acromioclavicular meniscus
Intrinsic Diagnoses • Impingement • Tendonitis • Bursitis • Rotator Cuff tear-complete • Rotator Cuff tear-partial • others
Intrinsic Diagnoses • Acromioclavicular joint irritation/arthritis • Glenohumeral joint osteoarthritis • Rheumatologic joint • Pigmented Villonodular synovitis • Chondrometaplasia • Tumors-giant cell, synovial sarcoma
Intrinsic Diagnoses • Instability/Subluxation-repetitive/chronic Atraumatic/multidirectional • Dislocation • Traumatic unidirectional • Biceps • Inflammation • Instability/subluxation • Tendonitis/avulsion
Intrinsic Diagnoses • History compatible • Physical exam compatible • Radiologic exam compatible • MRI/MRA compatible • Less so- blood work, others • Each is a piece of the puzzle
Physical Exam • Observation • Palpation • Range of Motion • Strength Test • Specific Tests for lesions • Hoppenfeld- Examination of the Extremies
Treatment • “ITIS”- inflammation- tendonitis, bursitis • Rest, avoidance, NSAIDS, injections, therapy • Osteoarthritis- above plus possible total shoulder replacement, ac joint • Rotator Cuff Tears-above +/- repair • Instability/Dislocation-+/- repair • Frozen Shoulder • Biceps Inflammation • The arthroscope has become an important tool for diagnosis and treatment in virtually all afflictions of the shoulder
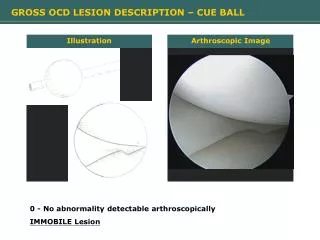
Arthroscope • Fiber optic device • Triangulate-the surgeon never sees the actual inside of the joint- it is projected upon a monitor and as such, the working tools, “triangulate’ to the point of focus • Minimally invasive • Less pain • Less rehabilitation
Treatment • Nsaids- short-term • Physical therapy • Injections • Surgery
Physical Therapy Treat Inflammation- Iontophoresis Treat Tight Areas Stretch Treat Weakness Strentghen- rotator cuff muscles scapular stabilizers
Injections • Must have correct diagnosis • Patient may have more than one pain location • Lidocaine Injection test • Areas- • Subacromial space • Glenohumeral joint • Ac joint • Bicipital sheath
Shoulder Pain-traditionally was treated with long delays in surgical intervention-Why? • Shoulder pathology not well understood • Open repair required extensive incisions • Rehabilitation was long • Most importantly, in times past, the primary care givers was, in general, “under-the-impression” that shoulder surgical intervention was not that effective
Arthroscopic Interventionutilized in • Impingement-bursitis, tendonitis • Rotator cuff tears • Instability or dislocation • AC joint arthritis • And yes even in Osteoarthritis
Arthroscope has allowed for the further identification of subtle shoulder pathology, previously not identified • See articles- 1) Bennett WF. Subscapularis, Medial and Lateral Head Coracohumeral Ligament Insertion Anatomy: Arthroscopic Appearance and Incidence of "Hidden" Rotator Interval Lesions. Arthroscopy. 2001 Feb. 17(2) 173-180 2) Bennett WF. Visualization of the Anatomy of the Rotator Interval. Arthroscopy. 2001 17 107-111
Arthroscopic Prospective outcomes are now Published • See Articles- Bennett WF: Arthroscopic Repair of Bennett WF: Arthroscopic Repair of Complete Anterosuperior Rotator Cuff Tears. 2 Year Follow-up. Arthroscopy, January 2003 Bennett WF: Arthroscopic Repair of Complete Subscapularis Tears. 2 Year Follow-up. Arthroscopy, February 2003 Bennett WF: Arthroscopic Repair of Complete Supraspinatus Tears. 2 Year Follow-up. Arthroscopy, March 2003 Bennett WF: Arthroscopic Repair of Massive Rotator Cuff Tears. 2-Year Follow-up Arthroscopy, April 2003
Natural History of Rotator Cuff Tears • Recurrence of pain • Tears get bigger with time • Results of surgical intervention deteriorates with time • Muscle turns to fat • Tendon becomes inelastic
At this Point • Most recently anatomy surrounding the rotator cuff and its interrelationship with the bicipital sheath has been identified, clarified, classified, arthroscopic reapir techniques developed and outcome studies published. • At this point I will move to the details of clinical research that I have been performing for the last 12 years.