Download
1 / 44
1.3k likes | 2.53k Views
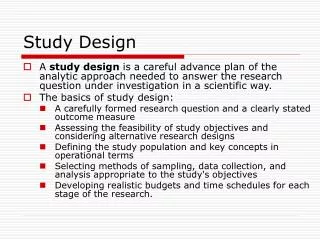
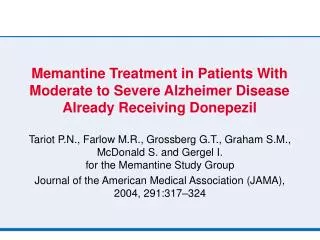
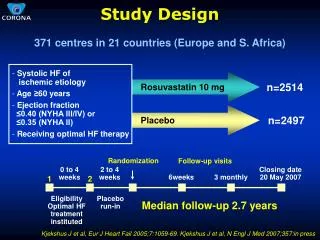
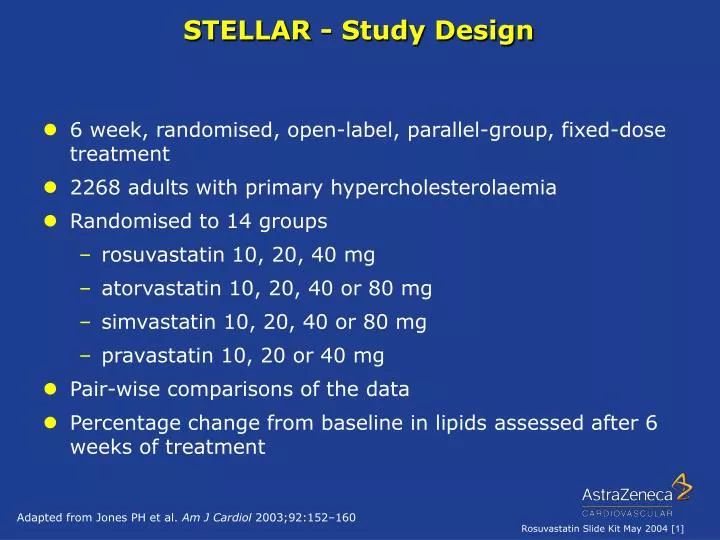
STELLAR - Study Design. 6 week, randomised, open-label, parallel-group, fixed-dose treatment 2268 adults with primary hypercholesterolaemia Randomised to 14 groups rosuvastatin 10, 20, 40 mg atorvastatin 10, 20, 40 or 80 mg simvastatin 10, 20, 40 or 80 mg

E N D
STELLAR - Study Design • 6 week, randomised, open-label, parallel-group, fixed-dose treatment • 2268 adults with primary hypercholesterolaemia • Randomised to 14 groups • rosuvastatin 10, 20, 40 mg • atorvastatin 10, 20, 40 or 80 mg • simvastatin 10, 20, 40 or 80 mg • pravastatin 10, 20 or 40 mg • Pair-wise comparisons of the data • Percentage change from baseline in lipids assessed after 6 weeks of treatment Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
10 mg 20 mg 40 mg 80 mg STELLAR - Pair-wise Comparisons 10 mg 20 mg 40 mg Rosuvastatin Atorvastatin 10 mg 20 mg 40 mg 80 mg 10 mg 20 mg 40 mg Rosuvastatin Simvastatin 10 mg 20 mg 40 mg Rosuvastatin 40 mg Pravastatin 10 mg 20 mg Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
Dose, mg (log scale) 40 10 20 80 Change in LDL-C from baseline (%) 0 –10 X –20 X –30 n=485 X –40 X n=648 X –50 * n=634 n=473 † ‡ –60 Rosuvastatin versus Comparators:LDL-C Efficacy Across the Dose RangeThe STELLAR Study Rosuvastatin Atorvastatin Simvastatin Pravastatin *p<0.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg †p<0.002 vs atorvastatin 20, 40 mg; simvastatin 20, 40, 80 mg; pravastatin 20, 40 mg ‡p<0.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
Change in LDL-C from baseline (%) 0 –5 –10 –15 –20 –25 –30 –35 –40 –45 –50 –55 –60 20 mg † 40 mg ‡ 10 mg * 10 mg 20 mg 40 mg 80 mg Rosuvastatin Atorvastatin Simvastatin 10 mg 20 mg 40 mg 80 mg Pravastatin 40 mg 10 mg 20 mg Rosuvastatin 10 mg (–46%) Rosuvastatin versus Comparators: LDL-C Efficacy at Low DoseThe STELLAR Study *p<0.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg †p<0.002 vs atorvastatin 20, 40 mg; simvastatin 20, 40, 80 mg; pravastatin 20, 40 mg ‡p<0.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
12 weeks 12 weeks 6 weeks 6 weeks 8 weeks 8 weeks Pooled data Pooled data STELLAR STELLAR MERCURY I MERCURY I Change in LDL-C from baseline (%) Jones Schuster Davidson Schwartz Olsson Blasetto 0 n=129 n=128 n=129 n=128 n=127 n=127 n=127 n=127 n=132 n=132 n=139 n=139 n=389 n=389 n=393 n=393 n=158 n=158 n=539 n=539 n=529 n=529 n=529 n=529 n=156 –10 –20 –30 –35 –35 –36 –37 –37 –39 –40 –43 –46 –47 –47 –47 * –50 * * –50 * * * –60 Rosuvastatin 10 mg Atorvastatin 10 mg Rosuvastatin versus Atorvastatin Consistent LDL-C Reduction at Low Dose *p<0.001 vs atorvastatin Jones PH et al. Am J Cardiol 2003;92:152–160 Schuster H et al. Am Heart J 2004; 147: 705-712 Davidson M et al. Am J Cardiol2002;89:268–75 Schwartz G et al. Am Heart J 2004: In Press Olsson AG et al. Am Heart J 2002;144:1044–51 Blasetto JW et al. Am J Cardiol 2003;91(Suppl):3C–10C
Rosuvastatin 10 mg versus Atorvastatin 20 mg Provides Greater LDL-C Reductions 6 weeks 8 weeks MERCURY I Schuster STELLAR Jones Jukema Franken Change in LDL-C from baseline (%) 0 n=156 n=155 n=230 n=231 n=128 n=131 n=539 n=925 -10 -20 -30 -38 -41 -40 -43 -44 -44 -46 -46 -47 * ns * -50 ** Rosuvastatin 10 mg Atorvastatin 20 mg -60 *p<0.05, **p<0.001 vs atorvastatin 20 mg Jones PH et al. Am J Cardiol 2003;92:152–160. Schuster H et al. Am Heart J 2004;147:705–712. Franken A et al. Atherosclerosis Supplements 2004; 5 (1): 118 Abs M.513. Jukema J et al.Atherosclerosis Supplements 2004; 5 (1): 125 Abs M.542.
Rosuvastatin versus Atorvastatin Achievement of LDL-C Goals at Low Dose 100% Rosuvastatin 10 mg # Atorvastatin 10 mg 80% Atorvastatin 20 mg * 77% 67% 66% 60% * 57% European LDL-C goal (%) Patients achieving 2003 52% 40% 36% 20% 13% n=538 n=529 n=925 n=389 n=393 n=201 n=196 0% All patients All patients Patients with CVD or type 2 diabetes 8 weeks MERCURY I Schuster1 12 weeks Pooled data Kritharides2 Rosuvastatin 10 mg vs atorvastatin 10 and 20 mg; patients achieving 2003 European LDL-C goals‡ ‡LDL-C <3mmol/l (115mg/dl) in general;<2.5mmol/l (97mg/dl) for patients with clinically established CVD or type 2 diabetes #p<0.001 vs atorvastatin 10 mg & 20 mg *p<0.001 vs atorvastatin 10 mg 1. Schuster H & Fox J. Exp Opin Pharmacother 2004;5:1187-1200 2. Kritharides L. Eur Heart J Suppl 2004; 6(Suppl A): A12-A18
Rosuvastatin vs Simvastatin and PravastatinAchievement of LDL-C Goals at Low Dose European LDL-C goal (%) Patients achieving 2003 Rosuvastatin 10 mg vs simvastatin 20 mg and pravastatin 20 & 40 mg; patients achieving 2003 European LDL-C goals‡ 100% Rosuvastatin Simvastatin # * 80% Pravastatin 77% 74% * 60% 55% 49% 40% 38% 37% 20% 12% 10mg 20mg 10mg 20mg 40mg 11% 3% 20mg 10mg 20mg n=74 n=538 n=543 n=521 n=226 n=249 n=252 n=64 n=86 0% 20mg All patients All patients Patients with CVD or type 2 diabetes 8 weeks MERCURY I Schuster1 12 weeks Pooled data Kritharides2 ‡LDL-C <3mmol/l (115mg/dl) in general;<2.5mmol/l (97mg/dl) for patients with clinically established CVD or type 2 diabetes #p<0.001 vs simvastatin & pravastatin *p<0.001 vs simvastatin & pravastatin 1. Schuster H & Fox J. Exp Opin Pharmacother 2004;5:1187-1200 2. Kritharides L. Eur Heart J Suppl 2004; 6(Suppl A): A12-A18
Rosuvastatin versus other statinsAchievement of LDL-C Goals Across Dose Range 100% † # 87% Atorvastatin 83% Simvastatin 80% * 75% Pravastatin 72% 69% 66% 60% 58% European LDL-C goal (%) Patients achieving 2003 48% 44% 40% 36% n=925 n=189 22% 20% 20% 12% 3% 0% 10 20 40 10 20 40 80 10 20 40 80 10 20 40 Dose (mg) Patients achieving 2003 European LDL-C goals‡ ‡LDL-C <3mmol/l (115mg/dl) in general; <2.5mmol/l (97mg/dl) for patients with clinically established CVD or type 2 diabetes Rosuvastatin *p<0.002 vs atorvastatin 10 mg; simvastatin 10, 20, 40 mg; pravastatin 10, 20, 40 mg †p<0.002 vs atorvastatin 20 mg; simvastatin 20, 40 mg; pravastatin 20, 40 mg #p<0.002 vs atorvastatin 40 mg; simvastatin 40, 80 mg; pravastatin 40 mg Kritharides L. Eur Heart J Suppl 2004; 6(Suppl A): A12-A18
* 100 40 mg 90 20 mg 80 mg 80 40 mg 10 mg 20 mg 70 60 Patients achieving LDL-C goals (%) 10 mg 50 96% 82% 87% 40 59% 30 20 10 n=106 n=116 0 Rosuvastatin Atorvastatin Rosuvastatin versus Atorvastatin Achievement of LDL-C Goal Across Dose Range Patients achieving NCEP ATP-II LDL-C goals over 52 weeks *p=0.006 rosuvastatin 10–40 mg vs atorvastatin 10–80 mg Olsson AG et al. Am Heart J 2002;144:1044–51 Schuster H. Cardiology 2003;99:126–139
Rosuvastatin versus Atorvastatin Achievement of LDL-C Goal Across Dose Range Patients achieving 2003 European LDL-C goal (<2.5mmmol/l)† 100 * 90% 90 40 mg 18 weeks 83% 80 mg 78% 20 mg 12 weeks 80 78% 77% 40 mg 70% 70 60 Patients achieving 2003 European LDL-C goal by dose (%) 50 6 weeks 10 mg 20 mg 40 30 20 10 n=131 n=132 0 Atorvastatin Rosuvastatin *p=0.05 rosuvastatin 40mg vs atorvastatin 80 mg †patients with type 2 diabetes and dyslipidaemia Adapted from Franken A, Atherosclerosis Supplements 2004; 5 (1): 118 Abs M.513
Change in HD-C from baseline (%) Rosuvastatin 12 Atorvastatin † * 10 n=473 ns 8 6 4 n=634 2 0 20 40 80 10 Dose (mg); log scale Rosuvastatin versus Atorvastatin Change in HDL-CThe STELLAR Study *p<0.002 vs atorvastatin 20, 40 and 80 mg †p<0.002 vs atorvastatin 40 and 80 mg Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
Rosuvastatin Atorvastatin † 9.5 ‡ 9.6 Simvastatin 12 * 7.7 Pravastatin 6.8 10 6.0 5.7 5.6 5.3 5.2 4.8 4.4 4.4 8 3.2 6 2.1 4 2 10 20 40 10 20 40 80 10 20 40 80 10 20 40 0 Dose (mg) Rosuvastatin versus Comparators Change in HDL-CTheSTELLAR Study Change in HD-C from baseline (%) *p<0.002 vs pravastatin 10 mg †p<0.002 vs atorvastatin 20, 40, 80 mg; simvastatin 40 mg; pravastatin 20, 40 mg ‡p<0.002 vs atorvastatin 40, 80 mg; simvastatin 40 mg; pravastatin 40 mg Observed data in ITT population Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
0 10 20 40 10 20 40 80 10 20 40 Change in TG from baseline (%) 10 20 40 80 –5 –7.7 –8.2 –10 –11.9 –13.2 –15 –14.8 –17.6 –18.2 –20 Rosuvastatin –19.8 * –20.0 Atorvastatin –22.6 Simvastatin –25 –23.7 † Pravastatin –26.1 ‡ –26.8 –30 –28.2 Rosuvastatin versus Comparators Change in TriglyceridesThe STELLAR Study Dose (mg) *p<0.002 vs pravastatin 10, 20 mg †p<0.002 vs simvastatin 40 mg; pravastatin 20, 40 mg ‡p<0.002 vs simvastatin 40 mg; pravastatin 40 mg Adapted from Jones PH et al. Am J Cardiol 2003;92:152–160
Rosuvastatin Efficacy Summary • Rosuvastatin is the most effective statin at lowering LDL-C • Rosuvastatin has demonstrated highly effective reductions in LDL-C of up to 63% • Rosuvastatin lowers LDL-C significantly more than the same and some higher doses of other currently marketed statins • Rosuvastatin 10 mg lowers LDL-C significantly more than atorvastatin 10 and 20 mg • Rosuvastatin 10 mg enables significantly more patients to achieve their LDL-C goal than the most commonly prescribed doses of other currently marketed statins, thereby reducing the need to titrate to higher doses • Rosuvastatin produces a significant increase in HDL-C which, unlike atorvastatin, is maintained across the dose range
Rosuvastatin Tolerability and Safety Adverse event profile Liver Effects Muscle Effects Renal Effects
Rosuvastatin Clinical Studies Included a Wide Range of Patients • Range of patients reflecting those seen in general medical practice • 53% male; 47% female (including women of childbearing age) • no upper age limit (31% ≥65 years) • 17% with type 2 diabetes • 52% with hypertension • 36% with overt cardiovascular disease • 44% with mild renal impairment (8% moderate renal impairment)
Rosuvastatin Tolerability and Safety - Adverse Events • Rosuvastatin is generally well tolerated with an adverse event profile similar to currently marketed statins • Most common related adverse events - myalgia, asthenia, abdominal pain, nausea; these are generally mild and transient • Well tolerated regardless of age, sex, ethnicity, presence of co-morbidities or concomitant medications • Similar number of adverse events leading to withdrawal (<3%) as other currently marketed statins Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K
8 7 6 5 Patients (%) 4 3.2% 2.9% 2.5% 2.5% 3 2 10–80 mg 10–40 mg 10–80 mg 10–40 mg 1 0 atorvastatin rosuvastatin simvastatin pravastatin (n=3074) (n=2899) (n=1457) (n=1278) Rosuvastatin Tolerability and Safety - Withdrawals due to Adverse Events Percentage of patients with an adverse event leading to withdrawal Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K
Rosuvastatin Tolerability and Safety - Liver Effects • Elevations in liver transaminase levels are an infrequent but recognized complication of treatment with statins • Low incidence of clinically significant increases in serum transaminases* with rosuvastatin 10–40 mg of 0.2% which compares well with that seen with other currently marketed statins1 • As with other statins: • liver function tests recommended • caution in patients who consume excessive quantities of alcohol and/or have a history of liver disease • contraindicated in patients with active liver disease *ALT >3 x ULN on 2 successive occasions 1. Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K Please refer to local Prescribing Information
Rosuvastatin (10, 20, 40 mg) Atorvastatin (10, 20, 40, 80 mg) Simvastatin (40, 80 mg) 3.0 Lovastatin (20, 40, 80 mg) Occurrence ofALT >3×ULN (%) 2.5 Fluvastatin (20, 40, 80 mg) 2.0 1.5 1.0 0.5 0.0 20 30 40 50 60 70 LDL-C reduction (%) Rosuvastatin Benefit:Risk – Liver Effects ALT >3 × ULN: Frequency by LDL-C Reduction Persistent elevation is elevation to >3 x ULN on 2 successive occasions Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K
Rosuvastatin Tolerability and Safety - Muscle Effects • As with other statins, effects on skeletal muscle, e.g. uncomplicated myalgia, myopathy and, rarely, rhabdomyolysis have been reported in patients treated with rosuvastatin • Frequency of treatment-related myopathy*in clinical trials was <0.1% in patients treated with rosuvastatin up to 40 mg which compares well with that seen with other currently marketed statins1 • Frequency of rhabdomyolysis with rosuvastatin is similar to that reported for the other marketed statins2 • *defined as CK >10 ULN plus muscle symptoms • Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K • Data on File • Please refer to local Prescribing Information
Rosuvastatin (10, 20, 40 mg) Atorvastatin (10, 20, 40, 80 mg) 3.0 Simvastatin (40, 80 mg) Occurrence of CK >10×ULN (%) 2.5 Pravastatin (20, 40 mg) Cerivastatin (0.2, 0.3, 0.4, 0.8 mg) 2.0 1.5 1.0 0.5 0.0 20 30 40 50 60 70 LDL-C reduction (%) Rosuvastatin Benefit:Risk - Muscle EffectsCK >10 x ULN: Frequency by LDL-C Reduction Brewer HB. Am J Cardiol 2003;92(Suppl):23K–29K
Tubular proteinuria Glomerular proteinuria Normal Blood Blood Blood Glomerulus Tubule Bladder Waste Products High molecular weight proteins (includes large amounts of albumin) Low molecular weight proteins (includes small amounts of albumin) Tolerability and Safety - Renal Effects Types of Proteinuria
Rosuvastatin Tolerability and Safety - Proteinuria • During the clinical development programme proteinuria* was observed in a small number of patients receiving all statin therapies studied and placebo1 • This observation was thoroughly investigated in rosuvastatin patients. It was found to be usually transient, often resolved on continued treatment and not predictive of acute or progressive renal disease1 • Proteinuria observed with rosuvastatin was tubular (reduced reabsorption of normally filtered proteins) in origin1 • Development of this tubular proteinuria is likely to be a consequence of the pharmacological action of rosuvastatin, ie. inhibition of HMG-CoA reductase, in the renal tubular cell2,3 • Highly effective inhibition of HMG-CoA reductase together with a greater degree of renal excretion contribute to this being seen with rosuvastatin *dipstick positive proteinuria defined as a shift from no protein or trace at baseline to ≥++ 1. Vidt DG et al. Cardiology 2004;102:52-60 2. Sidaway J et al. Toxicology Letters 2003;144 (supplement 1):s96 Abs 353 3. Verhulst A et al. Presented at American Society of Nephrology Nov 2003 Please refer to local Prescribing Information
Rosuvastatin Tolerability and Safety - ProteinuriaFrequency of Proteinuria* *dipstick positive proteinuria defined as a shift from no protein or trace at baseline to ≥++ Vidt DG et al. Cardiology 2004;102:52-60
Rosuvastatin Tolerability and Safety – Maintenance of Renal Function • In over 6000 patients receiving rosuvastatin (10-40mg) for up to 3.8 years, renal function† was maintained or tended to improve slightly • This was evident in all patient groups studied, including those at risk of progressive renal disease such as the elderly, patients with type 2 diabetes, hypertension or with pre-existing renal dysfunction/proteinuria and also in those who developed a positive urine dipstick test during the period of treatment* *dipstick positive proteinuria defined as a shift from no protein or trace at baseline to ≥++ †assessed using derived GFR measurements Vidt DG et al. Cardiology 2004;102:52-60 Please refer to local Prescribing Information
Rosuvastatin Tolerability and Safety – Maintenance of Renal Function Assessed by GFR Change in GFR in patients receiving placebo or rosuvastatin in short-term controlled clinical trials and long-term open-label treatment Rosuvastatin 10 mg Rosuvastatin 20 mg Rosuvastatin 40 mg 72 n=2107 (40 mg) Placebo 71 71 n=109 (40 mg) n=1432 (20 mg) 70 70 70 69 n=119 (20 mg) 69 n=2909 (10 mg) 68 68 68 Change in GFR (ml/min/1.73m2) n=893 (10 mg) 67 67 67 n=371 (placebo) 66 66 65 64 64 64 64 63 Baseline GFR On-treatment Baseline GFR On-treatment GFR GFR Short-term controlled clinical trials (~8 weeks) Long-term open label treatment (>96 weeks) p<0.001 for rosuvastatin 10 mg, 20 mg and 40 mg vs baseline for both short and long-term treatment Vidt DG et al. Cardiology 2004;102:52-60
Rosuvastatin Tolerability and Safety – Maintenance of Renal Function in Different Patient Groups Change in GFR in patients receiving long-term (>96 weeks) with rosuvastatin 10 mg 6 5 4 Mean change in GFR (ml/min/1.73m2) 3 2 1 n=590 n=836 n=413 n=537 n=243 n=650 n=356 n=303 n=480 n=832 n=46 n=61 0 >65 M N -ve <65 N Y F Y +ve >60 <60 Age, years Gender Hypertension GFR‡ Type 2 Urine dipstick diabetes protein† ‡ml/min/1.73m2 † negative is ‘none or trace’ positive is >1+ at baseline Vidt DG et al. Cardiology 2004;102:52-60
Rosuvastatin Tolerability and Safety - Renal Safety Summary • Rosuvastatin 10–40 mg is well tolerated from the renal perspective • Proteinuria* was seen in a small number of patients receiving all statin therapies studied and placebo • Proteinuria observed with rosuvastatin was thoroughly evaluated and found to be mostly tubular, usually transient, often resolved on continued treatment and not predictive of acute or progressive renal disease • Renal function was maintained or tended to improve slightly with long-term treatment *dipstick positive proteinuria defined as a shift from no protein or trace at baseline to ≥++
Rosuvastatin - Overall Tolerability and Safety Summary • Tolerability profile has been well-researched in a large number of patients representing ‘real population’ • Overall tolerability profile of rosuvastatin comparable with currently marketed statins • Well tolerated with a low rate of withdrawals due to adverse events (<3%) • Adverse events usually mild and transient • Low incidence of myopathy and of clinically significant increases in serum transaminases with rosuvastatin 10–40 mg, comparable with currently marketed statins • Renal function was maintained or tended to improve slightly with long-term treatment • Favourable benefit–risk profile
Rosuvastatin - Experience Since Launch As of end April 2004 • Rosuvastatin is approved in over 50 countries • >4 million prescriptions issued • >1.5 million patients treated • Benefit–risk profile is consistent with that seen in the clinical development programme and compares favourably with other currently marketed statins
Pharmacokinetic Profile of Selected Statins *Elimination T1/2 of drug and metabolites, if any. CRESTOR (rosuvastatin calcium) Prescribing Information. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2003. Atorvastatin Calcium Prescribing Information 2002,Pfizer Inc, NY, NY; Simvastatin Prescribing Information, Merck & Co., Inc., Whitehouse Station, NJ; Pravastatin Prescribing Information 2003, Bristol-Meyers Squibb Company, Princeton, NJ.
Rosuvastatin - Limited Drug–Drug Interactions • Interactions of no clinical significance: • drugs where metabolism involves cytochrome P450 such as fluconazole, ketoconazole and traconazole • fenofibrate • digoxin • Interactions with limited clinical significance: • antacid - 50% rosuvastatin levels • erythromycin non-significant in rosuvastatin plasma levels • Interactions of clinical significance: • oral contraceptive pill - ethinyl oestradiol and norgestrel levels which may affect choice of oral contraceptive use • gemfibrozil – 2x in rosuvastatin plasma levels. Combination not recommended • cyclosporin – 7x in rosuvastatin plasma levels. Combination contraindicated outside of USA • warfarin – INR – monitoring of INR required Please refer to local Prescribing Information
Rosuvastatin Pharmacokinetics in Special Populations • No clinically relevant PK differences: • between younger and elderly (age ≥65 years) • between men and women • between caucasian, hispanic, and black or afro-caribbean groups • in patients with mild to moderate renal impairment (creatinine clearance ≥30 mL/min/1.73m2) • PK differences which may influence dose selection: • 2-fold increase in AUC in Japanese in Japan and Chinese in Singapore compared with Caucasians in North America and Europe • increase in Cmax in moderate/severe hepatic impairment • 3-fold increase in Cmax in severe renal impairment (CLcr <30 mL/min/1.73m2) Please refer to local Prescribing Information
Rosuvastatin - Dosing and Administration • Usual start dose 10 mg • for all patients (new or switch) as it effectively gets most patients to their LDL-C goal • Dose range 10–40 mg • Maximum LDL-C response within 4 weeks • significant response within 2 weeks • Once daily, any time of day, with or without food Please refer to local Prescribing Information
Ongoing Clinical Development - the Rosuvastatin GALAXY ProgrammeTM • The GALAXY ProgrammeTM is a large, comprehensive, long-term and evolving global research initiative sponsored by AstraZeneca investigating cardiovascular risk reduction and patient outcomes with rosuvastatin • It has been designed to build on current thinking to address important unanswered questions in statin research • Includes studies investigating the effects of rosuvastatin on: • atherogenic lipid profile and inflammatory markers • atherosclerosis • outcomes • Will provide additional short- and long-term efficacy and safety data for rosuvastatin • Designed to help physicians to improve the management of patients with hypercholesterolaemia and others with or at risk of cardiovascular disease Schuster H & Fox J. Expert Opinion in Pharmacotherapy 2004;5:1187-1200
GALAXY ProgrammeTM Studies GALAXY ProgrammeTM studies with rosuvastatin, investigating: Atherogenic lipid profile +/- inflammatory markers Atherosclerosis Reduction in CV morbidity & mortality ORION METEOR ASTEROID AURORA CORONA JUPITER STELLAR MERCURY I MERCURY II ORBITAL DISCOVERY COMETS LUNAR PLUTO POLARIS PULSAR ECLIPSE EXPLORER Schuster H & Fox J. Exp Opin Pharmacother 2004;5:1187-1200
Rosuvastatin has the Largest Number of Outcomes Studies Ongoing at Launch 1. Schuster H & Fox J. Exp Opin Pharmacother 2004;5:1187-1200 2. Fellström B et al. Nephrol Dial Transplant 2003;18(Suppl 4):713 3. Ridker P. Circulation 2003;108:2292–2297
Rosuvastatin - Overall Summary • Rosuvastatin produces beneficial effects on key lipid parameters at low dose and across the dose range • rosuvastatin is the most effective statin at lowering LDL-C • rosuvastatin 10 mg reduces LDL-C more than the same and some higher doses of other currently marketed statins • more patients to LDL-C goal with rosuvastatin 10 mg than commonly prescribed doses of other currently marketed statins, avoiding the need to titrate to higher doses • HDL-C increases maintained across the dose range, unlike atorvastatin • Tolerability and safety profile similar to other currently marketed statins • Low potential for significant drug–drug interactions • A comprehensive clinical development programme is ongoing, including a large number of outcomes studies