Download
1 / 41
410 likes | 527 Views
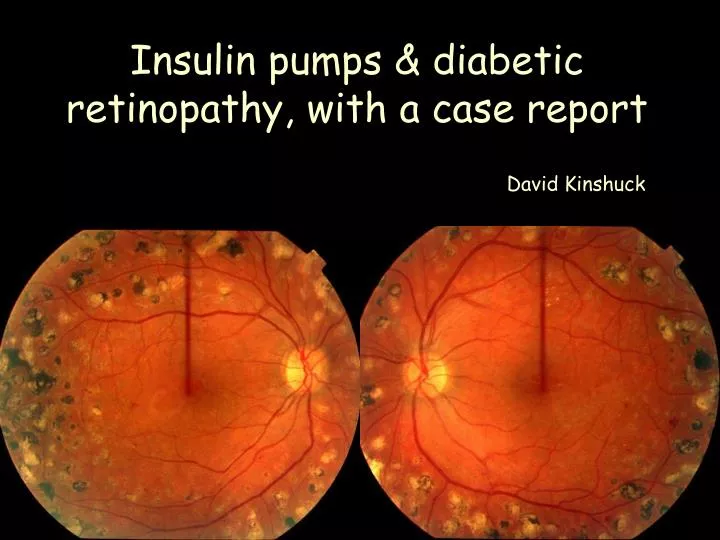
Insulin pumps & diabetic retinopathy, with a case report. David Kinshuck. Why is an ophthalmologist interested in insulin pumps?. Prevention or slowing of retinopathy retinopathy still disabling. This patient asked…would an insulin pump help me?.

E N D
Insulin pumps & diabetic retinopathy, with a case report David Kinshuck
Why is an ophthalmologist interested in insulin pumps? • Prevention or slowing of retinopathy • retinopathy still disabling
This patient asked…would an insulin pump help me? Answer given: help you & and your eyes if you achieve better control, and it is likely to improve your control,in the long term
What is an insulin pump? • Battery operated pump size of mobile phone • Worn eg round waist • Insulin in a vial is injected (through a tiny tube) into cannula inserted under the skin • pump is is programmed to deliver insulin constantly • patient determines rate • no other insulin injections, but still need to test glucose levels 4-6 x day (& adjust infusion rate) • ‘bolus’ insulin at meal times (amount size of meal) • basal rates otherwise (variable rate) • much more flexibility over your life • change cannula every 2 days (disconnect to swim etc)
1968 DOB, 1976 IDDM • 1998 background retinop, 6/5, 6/5 • 1999 proliferative, lots of laser, HbA1c 7.9% • works at ……………. husband very helpful/positive2000 indirect laser, sight worse = macular oedema, cannot drive • 6/24 then 6/60 both eyes • HbA1c 7.3%, but widely fluctuating sugars • Insulin pump 2000 • 2002 retinopathy not active, minor problems only, working 6/24, well, controlled Patient: 1
A bad result……. • Each patient with poor sight makes you think • was the laser OK? • diabetic control………..could we have done better? • European centres with good results have 2 monthly patient/DSN contact………how can we improve without this? • These clinics laser 1% diabetic patients, versus UK average 10% (Gouda, Holland) • 1/365 nurse/adult patient ratio (Holland), Good Hope 1/1333
Identifying progression of retinopathy • Exudates/oedema =leakage • New Vessels • An ‘early’ sign =haemorrhages • An increase in any of these • Photos useful for haemorrhages especially
Retinopathy is linked to: DCCT study 1% HbA1c = 37% progression rate
Retinopathy is linked to: 1mmHg = 1.1% progression rate
Retinopathy is linked to: Genetic = 25% Retinopathy Family history heart disease, stroke, blood pressure
Retinopathy is linked to: Smoking 20/day = 300% progression rate Passive smoker gets 25% of the smoke
Retinopathy is linked to: Statin reduces heart problems by 25-50% (estimate) Treat even if normal, especially if there are exudates
Retinopathy is linked to: ACE inhibitors reduce retinopathy by 50%
Retinopathy is linked to: Retinopathy progression
Retinopathy is linked to: Renal function decrease
Retinopathy is linked to: pregnancy
Progressing, HbA1c > 7.0%Why? • Suitable regime?………… young patients on bd insulin? • Basal bolus, but sugars fluctuate, hypos • This patient read about pumps and bought one herself • Do I mention pumps? • First patient’s retinopathy halted • Insulin pumpers web site, advice from retinopathy experts at European meetings
Balance motivation resources the wrong time or an unenthusiastic patient
Flexible dose insulin regime • Pump probably best for very dedicated (and rich) patients (HbA1c 6.0-7.0%), controversial • Best results are if you test your blood sugar 4-6 times a day, and adjust insulin • A typical new regime: lantus (glargine) longacting insulin for basal insulin; analogue for meals (lispro/novorapid) • 5% of patients are already on this new regime • Should be able to achieve HbA1c 7.0% with good nursing help, without dangerous hypos
Patient 2 • 1969 DOB, 1977 IDDM • professional, lives alone, sports++++ • 1995 background retinopathy, 6/5, 6/5 • 1995 proliferative, bd insulin • 1995-99 lots of laser, 6000/burns/eye • 2000 HbA1c 8.4% • 2000 vitreous haemorrhage • mediocre control/severe hypo • proliferation continues, laser • 2001 Insulin pump, well, controlled, happy • 2002 retinopathy not active • 6/9 driving/sports…some problems
Patient 3 • 1968 DOB, 1984 IDDM • 1998 background retinopathy, 6/5, 6/5 • 1999 HbA1c 9.7% (similar for years, alcohol++) • 2000 maculopathy lasered, 6/5 • 2001 proliferative, lots of laser, HbA1c 8.0 • 2002 struggled with pump, HbA1c 7.6 • Insulin pump, making wrong decisions re insulin, not in contact with other IDDM patients • got married, HbA1c 8.1 • ischaemic maculopathy, will get worse • ACE inhibitor • ?would starting pump while intellectual function better have helped
Patient 4 • 1966 DOB, 1971 IDDM • 1999 proliferative retinopathy++, 6/5, 6/5 • 1999, lots of laser, HbA1c 7.7%, • smoked and stopped re retinopathy • weight increased • ? Using insulin to diet/food issues • HbA1c 7.7%, but widely fluctuating sugars • Insulin pump, a real struggle • 2002 6/12, macular ischaemia still, 7.3% • retinopathy less active • would have had poor result without
What should we achieve? the wrong time unenthusiastic patient resources motivation Support people here Help change behaviour May have no choice to accept
Summary • 5 patients, have HbA1c about 1% less or fewer hypos • 4 with stable or nearly stable retinopathy • Many others not keen on pump • Hard work for 3, real struggle for 2 (& DSNs) • All have severe retinopathy scarring • Logically, better control earlier would be best • Improved decision making without retinopathy? (re patient adjusting own insulin) • 10 years behind European centres • Need 1-2 monthly contact with DSN • Desperately short of DSNs (& pumps)