Download
1 / 1
10 likes | 229 Views
IMPACT OF SEXUAL ABSTINENCE DURATION ON ICSI OUTCOME May Kew Loke and Pak Seng Wong Sunfert International Fertility Centre, Level 2 (East Wing), Sunway Medical Centre, No. 5, Jalan Lagoon Selatan, Bandar Sunway, 46150 Petaling Jaya, Malaysia. Introduction & Objective. Methods. Results.

E N D
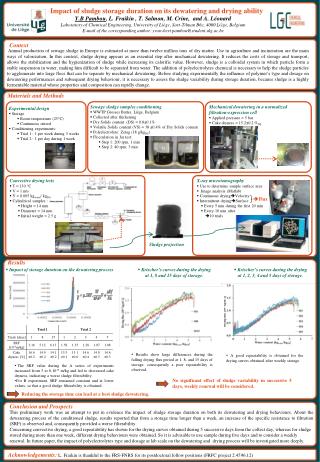
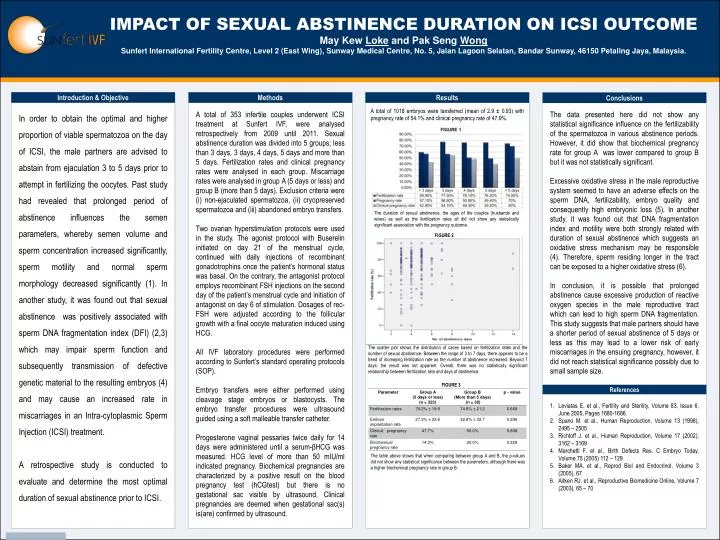
IMPACT OF SEXUAL ABSTINENCE DURATION ON ICSI OUTCOME May Kew Loke and Pak Seng WongSunfert International Fertility Centre, Level 2 (East Wing), Sunway Medical Centre, No. 5, Jalan Lagoon Selatan, Bandar Sunway, 46150 Petaling Jaya, Malaysia. Introduction & Objective Methods Results Conclusions In order to obtain the optimal and higher proportion of viable spermatozoa on the day of ICSI, the male partners are advised to abstain from ejaculation 3 to 5 days prior to attempt in fertilizing the oocytes. Past study had revealed that prolonged period of abstinence influences the semen parameters, whereby semen volume and sperm concentration increased significantly, sperm motility and normal sperm morphology decreased significantly (1). In another study, it was found out that sexual abstinence was positively associated with sperm DNA fragmentation index (DFI) (2,3) which may impair sperm function and subsequently transmission of defective genetic material to the resulting embryos (4) and may cause an increased rate in miscarriages in an Intra-cytoplasmic Sperm Injection (ICSI) treatment. A retrospective study is conducted to evaluate and determine the most optimal duration of sexual abstinence prior to ICSI. A total of 353 infertile couples underwent ICSI treatment at Sunfert IVF, were analysed retrospectively from 2009 until 2011. Sexual abstinence duration was divided into 5 groups; less than 3 days, 3 days, 4 days, 5 days and more than 5 days. Fertilization rates and clinical pregnancy rates were analysed in each group. Miscarriage rates were analysed in group A (5 days or less) and group B (more than 5 days). Exclusion criteria were (i) non-ejaculated spermatozoa, (ii) cryopreserved spermatozoa and (iii) abandoned embryo transfers. Two ovarian hyperstimulation protocols were used in the study. The agonist protocol with Buserelin initiated on day 21 of the menstrual cycle, continued with daily injections of recombinant gonadotrophins once the patient’s hormonal status was basal. On the contrary, the antagonist protocol employs recombinant FSH injections on the second day of the patient’s menstrual cycle and initiation of antagonist on day 6 of stimulation. Dosages of rec-FSH were adjusted according to the follicular growth with a final oocyte maturation induced using HCG. All IVF laboratory procedures were performed according to Sunfert’s standard operating protocols (SOP). Embryo transfers were either performed using cleavage stage embryos or blastocysts. The embryo transfer procedures were ultrasound guided using a soft malleable transfer catheter. Progesterone vaginal pessaries twice daily for 14 days were administered until a serum-βHCG was measured. HCG level of more than 50 mIU/ml indicated pregnancy. Biochemical pregnancies are characterized by a positive result on the blood pregnancy test (hCGtest) but there is no gestational sac visible by ultrasound. Clinical pregnancies are deemed when gestational sac(s) is(are) confirmed by ultrasound. The data presented here did not show any statistical significance influence on the fertilizability of the spermatozoa in various abstinence periods. However, it did show that biochemical pregnancy rate for group A was lower compared to group B but it was not statistically significant. Excessive oxidative stress in the male reproductive system seemed to have an adverse effects on the sperm DNA, fertilizability, embryo quality and consequently high embryonic loss (5). In another study, it was found out that DNA fragmentation index and motility were both strongly related with duration of sexual abstinence which suggests an oxidative stress mechanism may be responsible (4). Therefore, sperm residing longer in the tract can be exposed to a higher oxidative stress (6). In conclusion, it is possible that prolonged abstinence cause excessive production of reactive oxygen species in the male reproductive tract which can lead to high sperm DNA fragmentation. This study suggests that male partners should have a shorter period of sexual abstinence of 5 days or less as this may lead to a lower risk of early miscarriages in the ensuing pregnancy, however, it did not reach statistical significance possibly due to small sample size. A total of 1018 embryos were tansferred (mean of 2.9 ± 0.93) with pregnancy rate of 54.1% and clinical pregnancy rate of 47.9%. The duration of sexual abstinence, the ages of the couples (husbands and wives) as well as the fertilization rates all did not show any statistically significant association with the pregnancy outcome. FIGURE 2 The scatter plot shows the distribution of cases based on fertilization rates and the number of sexual abstinence. Between the range of 3 to 7 days, there appears to be a trend of increasing fertilization rate as the number of abstinence increased. Beyond 7 days, the result was not apparent. Overall, there was no statistically significant relationship between fertilization rate and days of abstinence. FIGURE 3 References • Leviatas E. et al., Fertility and Sterility, Volume 83, Issue 6, June 2005, Pages 1680-1686. • Spano M. et al., Human Reproduction, Volume 13 (1998), 2495 – 2505 • Richtoff J. et al., Human Reproduction, Volume 17 (2002), 3162 – 3169 • Marchetti F. et al., Birth Defects Res. C Embryo Today, Volume 75 (2005) 112 – 129 • Baker MA. et al., Reprod Biol and Endocrinol, Volume 3 (2005), 67 • Aitken RJ. et al., Reproductive Biomedicine Online, Volume 7 (2003), 65 – 70 The table above shows that when comparing between group A and B, the p-values did not show any statistical significance between the parameters, although there was a higher biochemical pregnancy rate in group B.