Download
1 / 66
680 likes | 931 Views
Anatomy, Physiology, Disorders and Overview of Diagnostic Tests of the Gastro-intestinal Tract. Tom Waterhouse. Learning Objectives. Anatomy and physiology of the GI Tract Gastro-Oesophageal Reflux Disease (GORD) Tests for diagnosis Motility disorders Diagnosis via oesophageal manometry.

E N D
Anatomy, Physiology, Disorders and Overview of Diagnostic Tests of the Gastro-intestinal Tract Tom Waterhouse
Learning Objectives • Anatomy and physiology of the GI Tract • Gastro-Oesophageal Reflux Disease (GORD) • Tests for diagnosis • Motility disorders • Diagnosis via oesophageal manometry
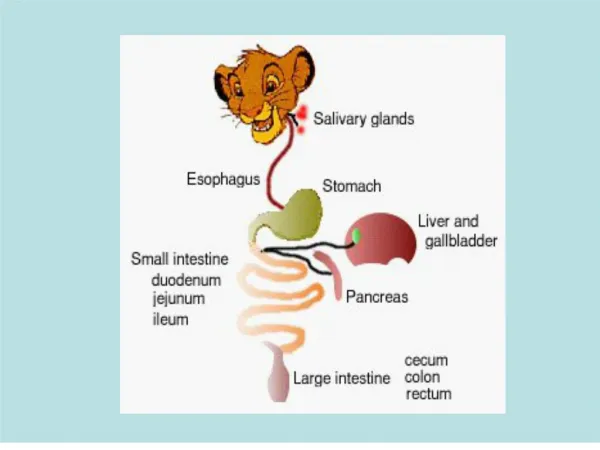
Anatomy and Physiology The GI Tract
Cross Section Lumen
Physical Digestion • Teeth - chewing • Tongue - shapes bolus • Saliva - lubricates bolus • Peristalsis + Segmentation • Longitudinal muscles + circular muscles • Stomach also has oblique muscles
Physical digestion - locations • Mouth - mastication • Oesophagus - peristalsis • Stomach - mastication & some peristalsis • Small intestine - segmentation & some peristalsis • Large intestine - peristalsis
Physical digestion - control valves • (Epiglottus) • Upper oesophageal sphincter (UOS) • Lower oesophageal sphincter (LOS) • Pyloric sphincter • (sphincter of Oddi) • Ileocecal valve • Anal Sphincters
Chemical Digestion • Carbohydrate digestion • Salivary amylase • Pancreatic amylase, lactase, sucrase, maltase etc • Protein digestion • Stomach • Denaturation by HCl, pepsin • Small Intestine • Trypsin, proteases, peptidases (pancreatic) • Bile salts (Sodium Bicarbonate) neutralise stomach acid • Fat Digestion • Lipase (pancreatic)
Anatomy and Physiology The oesophagus & stomach
Oesophagus • Muscular tube about 25cm long. • Upper third is skeletal type muscle. • Middle third is a mixture between skeletal and smooth muscle. • Lower third is smooth muscle. • When empty the oesophagus collapses into itself in longitudinal folds. These folds flatten out when food is in transit.
Oesophagus - 2 • The lower oesophageal sphincter separates the oesophagus from the stomach. • Extremely important for (in)digestion. • Stops acid coming back up from the stomach into the oesophagus and causing heartburn.
Stomach • Acidic, why? • Denature (unfold) proteins • Pepsinogen -> Pepsin
Quiz Time • What is the link between: Søren Sørensen
Acidity • What is pH? • Sorensen definition • p[H] = - log10[H+] • IUPAC • pH = - log10aH+
How is pH measured? • Circuit with two electrodes • Forms a cell when immersed • Nernst equation (reduction potential) • E = Eind - Eref = Eo + (RT/F x ln aH+) • E = measured voltage ( mV )E ind = voltage of indicator electrode (mV)E ref = voltage of reference electrode (mV)Eo = standard electrode potential (mV)R = gas constant ( 8.3144 J/K )T = absolute temperature ( K )F = Faraday's constant ( 96485.31 Coulombs )
How is pH measured(2)? • E = Eo + (RT/F x ln aH+) • E = Eo + (2.303 x RT/F x log10 aH+) • But pH = -log10 aH+ • pH = (Eo-E)/(2.303*RT/F) • Eo is constant, RT/F is constant at constant temperature (25.693 mV at 25oC) • Because activity is hard to quantify, pH is defined in ISO 31-8:1992, superceded by ISO/IEC 80000-9:2009 with reference to standard solutions
How is pH measured(3)? - Glass electrode • Glass sensing bulb • AgCl precipitate • 0.1 mol/L HCl for pH electrodes • internal AgCl/Calomel electrode • non-conductive body • reference electrode, usually same as 4 • Porous (eg ceramic) junction with studied solution
pH Electrodes • Glass • Broad accurate response (gold standard) • Fragile • Antimony • Robust • Smaller • Low cost • Linear between pH~1 and 10
Summary • Anatomy, Physiology of GI tract • What is acidity • How we measure it
Gastro-oesophageal Reflux Disease - GORD • Stomach contents ==> oesophagus via LOS. • pH (Stomach contents) normally < 4 • Typically pH~2. • Digestion of oesophagus! • 24 hour pH studies are performed to determine the levels of acid reflux.
GORD- Paediatric Complications/referral Criteria • Vomiting • Apnoea • De-saturation • Chronic cough • Recurrent chest infections • Failure to thrive/ gain weight • Colour changes
GORD- Adult Complications/referral Criteria • Vomiting • Regurgitation • Heartburn • Epigastric/ chest pain • Barrett’s epithelium
Oesophageal Ph Study - 1 • This can be performed on both adults and paediatrics. • Normally lasts 24 hours. • All medication that affects stomach acid is stopped prior to the investigation. • This can be up to 7 days in some instances. • Reports on the % time the ph measured drops below pH4. • Currently this tests involves the use of a naso-gastric catheter which is positioned in the oesophagus above the LOS.
Oesophageal Ph Study - 2 • Catheter placement is different for adults and paediatrics. • Adults- catheter is placed 5cm above the LOS. • Results from manometry. • HPZ Formula • Paediatrics- catheter is placed 2.5cm above the LOS. • Modified Strobel regression formula. • Occasionally checked using CXR.
Oesophageal Ph Study - 3 • Strobel Regression Fit (Paediatrics) • 5 + 0.252 x Child’s Height(cm)=___x 0.87 • HPZ formula for use in adults (Not commonly used): • Mx x 0.4 + 33 • (bone at top of rib cage to Xiphi-sternum) • Cx x 0.4 + 30 • (chin to Xiphi-sternum) • Add the above and divide by 2.
Oesophageal pH study - 4 • Calibration of the probe is performed using buffer solutions at pH values of 1 or 4 and 7. • Pre and post calibration is performed to check for any drift during the 24 hour period of the test.
Oesophageal Ph Study - 5 • Paediatric results based on published criteria from the RHSC (Glasgow). • Normal – below 5%. • Borderline – between 5 and 10%. • Abnormal – over 10%. • Adult results • In the West of Scotland and elsewhere, Demeester and Johnson scores above 14.72
WirelesspH monitoring systems • Medtronic developed an FDA approved wireless pH monitoring device, the Bravo pH Measurement System (now sold by Given Imaging, Ltd., Israel)
WirelesspH monitoring systems • Deployment is achieved with suction that pulls esophagealmucosa into a small well on the side of the probe, after whichthe metallic retaining bar is triggered to pierce the suctionedtissue and the placement catheter is withdrawn.
Acid Suppression Therapies • Gaviscon (infant & adult). • Ranitidine (H2 receptor antagonist) (Zantac). • Proton pump inhibitors. • Esomeprazole (Nexium). • Omeprazole (Losec). • Lansopazole (Zoton). • Pantoprazole (Protium). • Surgery - Nissen Fundoplication – tightening of the lower oesophageal sphincter.
Examples of Oesophageal Motility Disorders • Dysphagia • Oesophageal spasm • Achalasia • Hypercontractile distal oesophagus (nutcracker oesophagus) • Stricture • Carcinoma
Dysphagia • Defined as • the inability to swallow or • the sensation of the obstruction of food between mouth and stomach. • It can also be used to describe difficulty in swallowing and occurs from paralysis or a weakness of the muscles in the soft palate. • This can occur after stroke or in certain neurological disorders.
Oesophageal Spasm • Oesophageal spasm is characterised by repetitive non-peristaltic contractions of the oesophageal smooth muscles • Contractions can either be spontaneous or triggered by swallowing • Unknown cause
Achalasia • the absence of oesophageal peristalsis and a failure of the LOS to relax • unknown cause • may be associated with damage to the nerve fibers of the myenteric plexus supplying the oesophagus
Hypercontractile Distal Oesophagus • Commonly referred to as nutcracker oesophagus. • High distal pressures measured in the oesophagus above 180mmHg. • Can mimic cardiac chest pain. • Buscopan or glycerol trinitrate have been used as potential treatments.
Stricture - 1 • A stricture is a stenosis (narrowing) of the oesophageal lumen caused by the formation of fibrous scar tissue. • This can result from the inflammation caused by acid reflux from the stomach. About 50% of oesophageal strictures are associated with Barrett’s epithelium.