Download
1 / 27
300 likes | 580 Views
GASTRO INTESTINAL TRACT PHARMACOLOGY - 1. LECTURE 7. The Gastrointestinal Tract. Gastroesophageal Reflux Disease (GERD) Peptic Ulcer Disease (PUD) Duodenal Ulcer Nausea Emesis IBS Diarrhea Constipation. 0. Gastroesophageal Reflux Disease (GERD ).

E N D
GASTRO INTESTINAL TRACT PHARMACOLOGY - 1 LECTURE 7
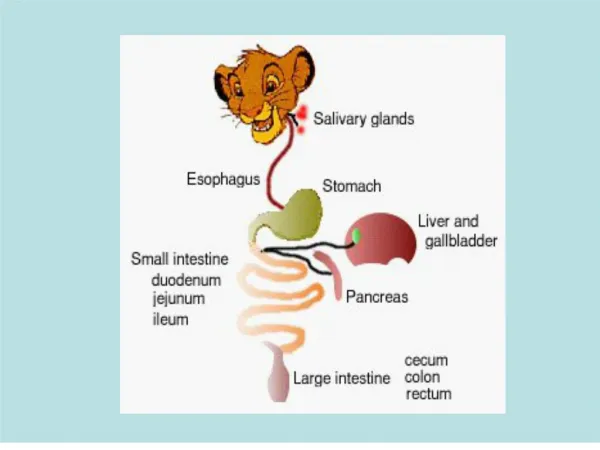
The Gastrointestinal Tract • Gastroesophageal Reflux Disease (GERD) • Peptic Ulcer Disease (PUD) • Duodenal Ulcer • Nausea • Emesis • IBS • Diarrhea • Constipation
0 Gastroesophageal Reflux Disease (GERD) GERD is when acid and pepsin from the stomach flows backward up into the esophagus often called heartburn; 1) Overproduction of acid/pepsin 2) Over relaxation of the Lower Esophageal Sphincter (LES); Complications; if not treated - severe chest pains, bleeding or a pre-malignant change in the lining of the esophagus called Barrett’s esophagus – can result in adenocarcinoma
General Considerations • Backflow of stomach acid into the esophagus • Esophagus is not equipped to handle stomach acid => scaring • Usual symptom is heartburn, an uncomfortable burning sensation behind the breastbone (MI often mistaken for GERD !) • More severe symptoms: difficulty swallowing, chest pain • Reflux into the throat can cause sore throat • Complications include esophageal erosions, esophageal ulcer and narrowing of the esophagus (esophageal stricture) • In some patients (~10%), the normal esophageal lining or epithelium may be replaced with abnormal (Barrett's) epithelium. This condition (Barrett's esophagus) has been linked to cancer of the esophagus. • Treatment : Generally antacids
PEPTIC ULCER • A benign lesion of gastric or duodenal mucosa occurring at a site where the mucosal epithelium is exposed to acid and pepsin; • 1) Excess acid production • 2) Intrinsic defect in the mucosal defense barrier • Average size ¼ and ½ inch in diameter • Peptic Ulcer Disease Affects All Age Groups • Men Have Twice The Risk as Women Do • Genetic Factors • Increase Acid Production and/or Decrease in Bicarbonate and PG Production
Duodenal Ulcer Gastric Ulcer HP NSAID Cancer (ZE) Other Pathophysiological Processes Involved in Duodenal and Gastric Ulcers
0 Strategies for Inhibiting Parietal Cell Acid Secretion CCK2 Gastrin Antagonists ↓ Ca+2 H2 Histamine Antagonists ↓cAMP H+ PP Gastric Lumen M3 Muscarinic Antagonists ↓ Ca+2
Cyclooxygenase Pathway Arachidonic Acid COX-1 Prostacycline Synthase Thromboxane Synthase Prostaglandin H2 Prostaglandin G2 Prostaglandin Synthase Prostacycline PG12 Thromboxane A2 Thromboxane B2 Prostacycline E2, F2 Prostacycline G2 RESULT = DECREASED ACID SECRETION & INCREASED MUCUS PRODUCTION
PPI- Omeprazole • Prototype H+, K+-ATPase inhibitor; A prodrug that needs a low pH to be active; • Irreversible (forms a covalent bond with the proton pump) - long lasting inhibition of acid production; • Profound reduction of gastric acid - elevates gastric pH significantly (20mg/day for 7days will decrease acid by 95%); • Highly protein bound; Metabolized by CYP2C & CYP3A; plasma half life of 1 to2 hours but long duration of action; Should be taken just prior to a meal and should NOT be taken with other acid-suppressing agents. • Others: esomeprazole, lansoprazole and pantoprazole
Histamine H2 Antagonists Decrease Acid Output Cimetidine (Tagamet) Ranitidine (Zantac) Famotidine (Pepcid) Nizatidine (Axid) Histamine cAMP H+ Protein Kinase PP K+ ATP H2 antagonist administered orally at arrow Histamine Antagonist 30 20 Acid Output (mEq/hr) 10 Time (hr) 1 2 3 4 5
0 Strategies for Inhibiting Parietal Cell Acid Secretion Gastrin CCK2 Ca2+ Prostaglandin Agonists EP3 (-) cAMP H+ Protein Kinase H2 PP Histamine K+ ATP Acetylcholine M3 Ca2+
0 Drugs for Acid-Peptic Disorders - Anticholinergics • Blockade of acetylcholine at muscarinic (M3/M1) receptors • Effectively blocks acid secretion (30 to 40%) • Limited by side-effects • Side-effects are typical of anticholinergics such as atropine • Dry mouth • Tachycardia • Blurred vision • Bowel discomfort (constipation) • Difficulty in urination
0 Drugs for Acid-Peptic Disorders - Anticholinergics • General muscarinic receptor antagonists (block all types of muscarinic receptors) • Atropine • Propantheline (Pro-Banthine) • Dicyclomine (Bentyl) • Selective M1 receptor antagonists • Pirenzepine • Telenzepine
Inhibits: Acid secretion Gastrin release Pepsin secretion Stimulates: Mucus secretion Bicarbonate secretion Mucosal blood flow 0 Drugs for Acid-Peptic Disorders – Prostaglandins (PGE2 & PGI2 ) • Act at prostaglandin EP3 receptors on parietal cells & on epithelial cells These compounds act by both inhibition of acid production and by increasing defense mechanisms • These compounds are also effective against direct damage produced by alcohol, aspirin and NSAIDs, and are therefore termed “cytoprotective”
0 Drugs for Acid-Peptic Disorders - Prostaglandins Misoprostol (Cytotec): • Synthetic Analog of Prostaglandin E1 • Anti-acid secretory • 0.1 to 0.2 mg results in 85% to 95% acid reduction • Prevention of NSAID gastric ulcers Side Effects • Diarrhea • Abortion • Exacerbate IBD and should not be given
0 Drugs for Acid-Peptic Disorders - Antacids • Antacids are weak bases that neutralize HCl in the stomach; • They do not decrease the secretion of acid, and in some cases increase secretion; • They do not suppress nocturnal acid secretion 1. Neutralize acid 2. Decrease acid load to duodenum 3. Diminish pepsin activity
0 Drugs for Acid-Peptic Disorders - Antacids • Magnesium hydroxide • Magnesium trisilicate • Magnesium-aluminum mixtures • Calcium carbonate • Sodium bicarbonate
0 Drugs for Acid-Peptic Disorders – Sucralfate (Carafate) • Sucralfate is a basic aluminum salt of sucrose octasulfate; • In the presence of acid (pH < 3-4) some of the aluminum ions dissociate and the resulting negatively charged molecule polymerizes to form a viscous paste-like substance; • This substance adheres strongly to gastric and duodenum mucosa and adheres even more strongly to partially denatured proteins such as those found at the base of the ulcer.
0 H. pylori Eradication Rates with Either Dual, Triple or Quad Therapy (1999)
0 H. pylori Eradication Rates with Either Dual, Triple or Quad Therapy (1999) GENERIC NAME DOSING DURATION CURE RATE (%) Dual therapies omeprazole 500 mg TID 14 days 70-80 amoxycillin 1,000 mg TID 14 days ranitidine 400 mg BID 28 days 73-84 clarithromycin 500 mg TID 14 days lansoprazole 30 mg TID 14 days 66-77 amoxycillin 1,000 mg TID 14 days
0 H. pylori Eradication Rates with Either Dual, Triple or Quad Therapy (1999) Cont. GENERIC NAME DOSING DURATION CURE RATE (%) Triple therapies lansoprazole 30 mg BID 14 days 86-92 amoxycillin 1,000 mg BID 14 day clarithromycin 500 mg BID 14 days
0 H. pylori Eradication Rates with Either Dual, Triple or Quad Therapy (1999) Cont. GENERIC NAME DOSING DURATION CURE RATE (%) Quad therapies bismuth subsalicylate Two tablets 7 days 85-95 525 mg QID metronidazole 250 mg QID 7 days tetracycline 500 mg QID 7 days omeprazole 20 mg BID 7 days or lansoprazole 30 mg BID 7 days
NEXT LECTURE Nausea Emesis IBS Diarrhea Constipation