Download

1 / 88
1.08k likes | 2.15k Views
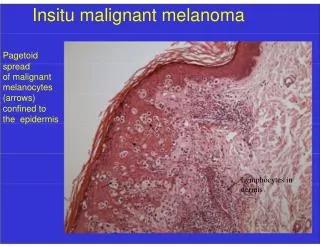
Surgical Treatment of Malignant Melanoma. Yağmur AYDIN, M.D. ,Asc. Prof. University of Istanbul, Cerrahpaşa Medical School Department of Plastic, Reconstructive and Aesthetic Surgery. Malignant Melanoma. Arise from melanocytes in basal layer in the epidermis

E N D
Surgical Treatment of Malignant Melanoma Yağmur AYDIN, M.D.,Asc. Prof. University of Istanbul, Cerrahpaşa Medical School Department of Plastic, Reconstructive and Aesthetic Surgery
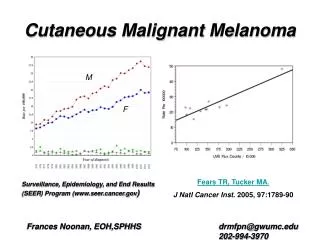
Malignant Melanoma • Arise from melanocytes in basal layer in the epidermis • The worst prognosis and morbidity in all skin cancers • Incidence is increasing by every year (% 6 per year) • accounts for only 4% of all skin cancers, but responsible for more than 77% of skin cancer deaths • Early detection and treatment important, because it reduces the mortality and increases survival • Prognosis ( 5 years) Local disease > % 90 Regional disease % 60 Distant metastasis % 5
Mostly arise from skin ( 95 % ) • But also found in the eyes, ears, GI tract, leptomeninges, and mucous membranes • Unknown primary or metastasis (3 %) • May develop in precursor melanocytic nevi(common, congenital, and atypical/dysplastic types (25 %) • Commonly arise from de-novo (not from a preexisting pigmented lesion)
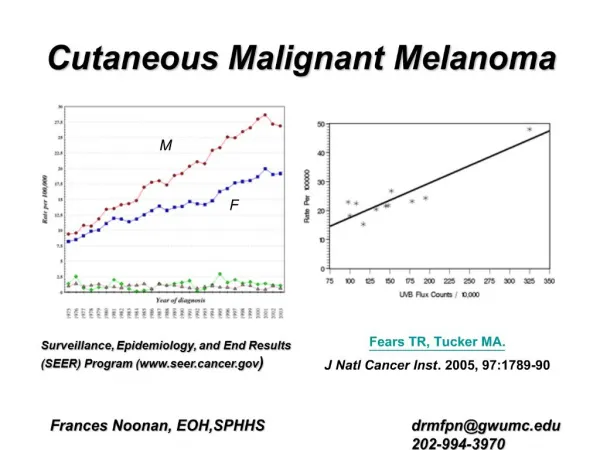
Causes • Melanoma tends to occur at sites of intermittent, intense sun exposure • an increased worldwide incidence in fair-complexioned individuals living in sunny climates and nearer the equator, suggesting a causative role for ultraviolet radiation.
Precursor Lesions • Atypical or Displastic nevi • Congenital nevi • Lentigo maligna • Acquired nevi
Risk Factors - I • Very fair skinned, particularly those with fair or red hair • Tendency to sun burn • Excessive childhood sun exposure and blistering childhood burns • Age : the incidence steadily rises with age. The highest incidence is in those over 80 • The more moles you have on your body, the higher your risk of melanoma (more than 100 Atypical or dysplastic nevi) The development of melanoma is multifactorial and appears to be related to multiple risk factors
Risk Factors -II • Born in a hot country, such as Australia or Israel • Malignant melanoma in the first degree relative (3-10 %) • Giant congenital nevi (5-40 ) • Second malignant melanoma (3-6 %) • Sunbeds (Solarium) • People who work outdoors and so are in the sun (sailors, farmers ..)
People who have risk factors should be follow and have preventive efforts
Early Diagnosis A changing mole is the most common warning sign for melanoma
Early Signs of Melanoma • The most common early sign of melanoma is pruritis • A,B,C,D,E warnin signs • Asymmetry: One half of the lesion does not match the other half. • Border irregularity: The edges are ragged, notched, or blurred. • Color variegation: Pigmentation is not uniform and may display shades of tan, brown, or black; white, reddish, or blue discoloration is of particular concern. • Diameter: A diameter greater than 6 mm is characteristic, although some melanomas may have smaller diameters; any growth in a nevus warrants an evaluation. • Evolving: Changes in the lesion over time • Bleeding and ulceration are late signs showing advanced disease
All suspected lesions are removed for histopathologic examination
Biopsy • Excision (Golden standard) • *İncision biopsy • *Punch biopsy • Partial thickness or shaving biopsies are contraindicated *All dermis layers should be removed
Balch CM, Houghton AN, Sober AJ, Soong S. Cutaneous Melanoma. St Louis QMP 1998
Melanoma is divided into the four major subtypes • Superficial spreading melanoma • Nodular melanoma • Lentigo Maligna Melanoma • Acral Lentiginous Melanoma
Superficial spreading melanoma • most common subtype of melanoma, occurring in approximately 70% of patients • most common on the trunk in men and women and on the legs in women • most commonly seen in individuals aged 30-50 years • Manifest as a flat or slightly elevated brown lesion with variegate pigmentation (ie, black, blue, pink, or white discoloration) • generally greater than 6 mm in diameter • Irregular asymmetric borders are characteristic
Superficial spreading melanoma • The most common melanoma mimickers are seborrheic keratoses Qenign keratinocytic proliferations) and traumatized nevi, which often present as a "bleeding mole." A mole showing severely atypical features may be clinically indistinguishable from a melanoma
Nodular Melanoma • Nodular melanoma is the second most common subtype of melanoma, occurs in 15-30% of patients • Seen most commonly on the legs and trunk • Rapid growth occurs over weeks to months • Lack of an identifiable in situ (or radial growth) phase • Responsible for most thick melanomas • Manifests as a dark brown-to-black papule or dome-shaped nodule, which may ulcerate and bleed with minor trauma • Tends to lack the typical ABCDE melanoma warning signs
Lentigo Maligna Melanoma • accounts for 4-15% of cutaneous melanoma cases • typically located on the head, neck, and arms (sun-damaged skin) of fair-skinned older individuals (average age 65 y) • grows slowly over 5-20 years • Only 5% to 8% of lentigo maligna are estimated to evolve to invasive melanoma. • Lentigo maligna appears as a tan to brown macule or patch with variation in pigment or areas of regression that appear hypopigmented clinically. • Lentigo maligna melanoma is characterized by nodular development within the precursor lesion.
Lentigo Maligna Melanoma Level II
Acral Melanoma • Acral lentiginous melanoma is the least common subtype, representing only 2% to 8% of melanoma in Caucasians, • It typically occurs on the palms or soles or beneath the nail plate (subungual variant). Irregular pigmentation, large size (>3 cm diameter), and plantar location are characteristic features of acral lentiginous melanoma.
Acral Melanoma • Subungual melanoma may be confused with a benign junctional nevus, pyogenic granuloma, or subungual hematoma. • Rapid onset of diftuse nail discoloration or a longitudinal pigmented band within the nail plate warrants biopsy of the nail matrix, from which these melanomas arise. • The additional presence of pigmentation in the proximal or lateral nail folds (Hutchinson's sign) is diagnostic of subungual melanoma