Download
1 / 37
370 likes | 381 Views
This article discusses the rare neoplasm of anorectal malignant melanoma, including its epidemiology, presentation, investigations, staging, prognosis, and treatment options such as surgery and adjuvant therapy.

E N D
A Revisit to AnorectalMalignant Melanoma (ARMM) Joint Hospital Surgical Grand Round 8 Nov 2014 Dr Jessie Chan Pamela Youde Nethersole Eastern Hospital
Outline • Introduction • Epidemiology • Presentation • Investigations • Staging • Prognosis • Treatment • Surgery • Adjuvant therapy
Introduction • Rare neoplasm • First reported by Moore in 1857 • Distinct biological and clinical entity from cutaneous melanoma with worse prognosis • No clear etiology elucidated • Arised from melanocytes distal to dentate line and extend proximally to rectum • Arised directly from melanocytes which present rarely in the mucosal epithelium of proximal anus or distal rectum
ARMM • <1% of all malignant melanomas • <4% of anal canal malignancies • Primary • Secondary • Metastasis from cutaneous melanoma (2%)
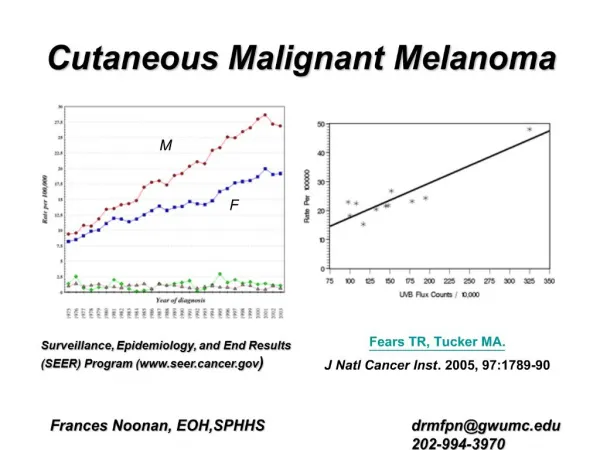
Epidemiology • Median age at presentation: 55 (range 29-92) • Reported incidence: 0.04 – 1.19% • No adequate population-based studies to draw definite conclusions for racial and gender difference
Presentation • Non-specific symptoms • PR bleeding • Anal pain, anal mass • Tenesmus, pruritus • Change in bowel habit • Symptoms of metastatic disease • Most common sites of metastases: inguinal / mesenteric / hypogastric / para-aortic lymph nodes, liver, lung, skin, brain • Weight loss, groin mass, pelvic mass, bowel obstruction • Incidental finding
Presentation • 80% lack obvious pigmentation • 20% histologically amelanotic
Presentation • Up to 60% with locoregional lymphatic spread (mesorectal, pelvic side wall, inguinal lymph nodes) • Up to 40% with distant metastasis
Investigations • Endoscopy and biopsy • Staging • Endoscopic ultrasound: role unclear • CT: regional lymphadenopathy, distant metastasis • PET scan: may be helpful
Staging • Cutaneous melanoma: AJCC TNM system • ARMM • Clinical staging • Stage I: local disease • Stage II: local disease with regional lymph nodes • Stage III: distant metastatic disease
Prognosis • Poor prognosis • Overall 5-year survival 3-22% • Survival <10 months with recurrent or metastatic disease
Prognosis • Good prognostic factors • Tumour thickness <2mm • Poor prognostic factors • Tumour thickness >3mm • Tumour site above dentate line • Lymphovascular / perineural invasion • Necrosis Wanebo HJ, Woodruff JM, Farr GH, et al. Anorectal melanoma. Cancer. 1981 Apr 1; 47(7):1891-900. Brady MS, Kavolius JP, Quan SH. Anorectal melanoma. A 64-year experience at Memorial Sloan-Kettering Cancer Center.Dis Colon Rectum. 1995 Feb; 38(2):146-51. Perez DR, Trakarnsanga A, Shia J, et al. Locoregional lymphadenectomy in the surgical management of anorectal melanoma. Ann Surg Oncol. 2013;20:2339-2344.
Treatment • Surgery • Wide local excision (WLE) • Abdominoperineal resection (APR) • Regional lymph node • Sentinel lymph node biopsy • Lymphadenectomy
Treatment • Adjuvant therapy • Systemic • Chemotherapy • Biochemotherapy • Interferon • Vaccine / immunotherapy • Local • Radiation therapy • Electrochemotherapy
Surgery • Mainstay of treatment • Controversies • APR vs local excision (LE) APR – en bloc excision with mesorectal lymph nodes ?oncological benefit • Inguinal lymphadenectomy
Surgery • Meta-analysis by Akihisa Matsuda et al in Annals of Surgery 2014 • 31 studies • 1006 patients • APR vs LE • Overall survival • Relapse-free survival • Local recurrence rate Akihisa Matsuda, Masao Miyashita, Satoshi Matsumoto, et al. Abdominoperineal Resection Provides Better Local Control But Equivalent Overall Survival to Local Excision of Anorectal Malignant Melanoma – A Systemic Review. Ann Surg. 2014; 00: 1-8.
APR vs LE • Overall survival – no difference (31 studies, N=1006)
APR vs LE • Recurrence-free survival – no difference (14 studies, N=328)
APR vs LE • Local recurrence rate – significantly lower in APR (13 studies)
Surgery • No survival benefit from APR over LE • Higher local recurrence from LE which could be managed by salvage surgery • Less complications and morbidities with LE • Better body image • Better urinary and sexual function • Minimal impact on bowel function • Minimizing morbidities and maximizing quality of life merits consideration in such an aggressive disease
Inguinal lymphadenectomy • Locoregional lymph node metastasis – no significant prognostic implication Perez DR, Trakarnsanga A, Shia J, et al. Locoregional lymphadenectomy in the surgical management of anorectal melanoma. Ann Surg Oncol. 2013;20:2339-2344.
Inguinal lymphadenectomy • Systemic dissemination with micrometastasis in distant organs occurs early with unfavourable prognosis • Prophylactic – no improvement in survival, increased risk of complications • Therapeutic – seems not to contribute to improvement of survival Perez DR, Trakarnsanga A, Shia J, et al. Locoregional lymphadenectomy in the surgical management of anorectal melanoma. Ann Surg Oncol. 2013;20:2339-2344.
Chemotherapy • Role remains unclear • ?Adjuvant • ?Palliative • Dacarbazine, cisplatin, vinblastine, vincristine, nimustine, bacillus Calmette-Guérin, levamisole, temozolomide • Single or combination – poor results
Interferon • Interferon alpha • Combination of direct activities and indirect immune-mediated effects • Parenteral route / intratumoural injection • No standard regimen established • Insufficient data
Biochemotherapy • Biologic agent (interferon, interleukin) + traditional cytotoxic chemotherapeutic agent • Longer disease-free and median survival in metastatic ARMM when compared with chemotherapy alone Kim K B, Sanguino A M, Hodges C, et al. Biochemotherapy in patients with metastatic anorectal mucosal melanoma. Cancer. 2004;100:1478–1483. Atkins MB, Lotze MT, Dutcher JP, et al. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and 1993. J Clin Oncol. 1999 Jul; 17(7):2105-16.
Biochemotherapy • Role • Best available adjuvant therapy after surgery • Considered in advanced or metastatic ARMM
Vaccine / Immunotherapy • Immunize against melanoma cell antigen • BRAF and cKIT mutations • Insufficient data • Area of significant research effort and may play an important part of the non-operative treatment of melanoma in the future
Radiation Therapy • Locoregional disease control • Primary lesion, inguinal and pericolic lymph nodes • Utility unclear, evidence conflicting
Radiation Therapy • Ballo et al • Local excision + post-op RT • Local control rate comparable with APR • 5-year local control rate: 74% • No improvement in survival • Moozar et al • Pre-op RT little effect on tumour burden • Post-op RT did not change local recurrence • No survival benefit Ballo MT, Gershenwald JE, Zagars GK, et al. Sphincter-sparing local excision and adjuvant radiation for anal-rectal melanoma.J Clin Oncol. 2002 Dec 1; 20(23):4555-8. Moozar KL, Wong CS, Couture J. Anorectal malignant melanoma: treatment with surgery or radiation therapy, or both.Can J Surg. 2003 Oct; 46(5):345-9.
Electrochemotherapy • Injection of chemotherapy directly into the lesions, followed by application of electric pulses using a needle electrode • Electrical stimulation to the tissues creating a transient permeabilization of the plasma membrane • Allows direct access of the chemotherapeutic agents into the cytosol of tumor cells • Known to provide effective local control for cutaneous melanoma
Electrochemotherapy • Convert APR to sphincter-preserving local excision • Overall success rate unclear Snoj M, Rudolf Z, Cemazar M,et al. Successful sphincter-saving treatment of anorectal malignant melanoma with electrochemotherapy, local excision and adjuvant brachytherapy.Anticancer Drugs. 2005 Mar; 16(3):345-8.
Summary • ARMM is a rare and highly malignant disease • Survival predicted by status of regional and distant metastasis but not method of surgery for local control • Minimizing surgical morbidities and maximizing quality of life should be the major consideration in formulating the treatment plan • Role of all adjuvant therapies is still unclear
References • P Carcoforo, M.T Raiji, G.M Palini, et al. Primary Anorectal Melanoma: An Update.J Cancer. 2012; 3:449-453. doi:10.7150/jca.5187. • Marc Singer and Matthew G. Mutch.Anal Melanoma.Clin Colon Rectal Surg. May 2006; 19(2): 78–87. • Akihisa Matsuda, Masao Miyashita, Satoshi Matsumoto, et al. Abdominoperineal Resection Provides Better Local Control But Equivalent Overall Survival to Local Excision of Anorectal Malignant Melanoma – A Systemic Review. Ann Surg. 2014; 00: 1-8. • Perez DR, Trakarnsanga A, Shia J, et al. Locoregional lymphadenectomy in the surgical management of anorectal melanoma. Ann Surg Oncol. 2013;20:2339-2344. • Wanebo HJ, Woodruff JM, Farr GH, et al. Anorectal melanoma. Cancer. 1981 Apr 1; 47(7):1891-900. • Brady MS, Kavolius JP, Quan SH. Anorectal melanoma. A 64-year experience at Memorial Sloan-Kettering Cancer Center.Dis Colon Rectum. 1995 Feb; 38(2):146-51.
References • Kim K B, Sanguino A M, Hodges C, et al. Biochemotherapy in patients with metastatic anorectal mucosal melanoma. Cancer. 2004;100:1478–1483. • Ulmer A, Metzger S, Fierlbeck G. Successful palliation of stenosing anorectal melanoma by intratumoral injections with natural interferon-β.Melanoma Res. 2002;12:395–398. • Atkins MB, Lotze MT, Dutcher JP, et al. High-dose recombinant interleukin 2 therapy for patients with metastatic melanoma: analysis of 270 patients treated between 1985 and 1993.J Clin Oncol. 1999 Jul; 17(7):2105-16. • Snoj M, Rudolf Z, Cemazar M,et al. Successful sphincter-saving treatment of anorectal malignant melanoma with electrochemotherapy, local excision and adjuvant brachytherapy.Anticancer Drugs. 2005 Mar; 16(3):345-8. • Ballo MT, Gershenwald JE, Zagars GK, et al. Sphincter-sparing local excision and adjuvant radiation for anal-rectal melanoma.J Clin Oncol. 2002 Dec 1; 20(23):4555-8. • Moozar KL, Wong CS, Couture J. Anorectal malignant melanoma: treatment with surgery or radiation therapy, or both.Can J Surg. 2003 Oct; 46(5):345-9.