Download
1 / 57
570 likes | 727 Views
THE AETNA & CIGNA SETTLEMENTS _________________________________ WHAT THEY MEAN TO YOU AND YOUR PRACTICE. The Problem. Improper and illegal reimbursement practices used by the managed care industry to delay or deny payment for: Bundling Downcoding Recoding Failure to recognize modifiers

E N D
THE AETNA & CIGNA SETTLEMENTS _________________________________ WHAT THEY MEAN TO YOU AND YOUR PRACTICE 1
The Problem • Improper and illegal reimbursement practices used by the managed care industry to delay or deny payment for: • Bundling • Downcoding • Recoding • Failure to recognize modifiers • Lack of disclosure • Breach of prompt pay laws 2 1
The MultiDistrict Litigation • MSSNY brought class action lawsuits against Aetna, Cigna, United Healthcare, Oxford, Empire Blue Cross Blue Shield and Excellus. • Numerous State Medical Societies brought lawsuits based on state law theories . • Meanwhile, several other State and County Medical Societies brought class action lawsuits against large for-profit managed care companies including but not limited to Aetna, Cigna and United Healthcare based on the Federal Anti-Racketeering statue (“RICO”). • MSSNY’s Lawsuits against Aetna, Cigna and United Healthcare were removed to federal court. • As a result, MSSNY’s lawsuits were consolidated with the RICO lawsuits in U.S. District Court in Miami Florida. • Pending before Judge Frederico Moreno. 1 3
The MultiDistrict Litigation (cont.) • MSSNY’s lawsuits are for the most part based on New York State General Business Laws and Public Health Laws. • The “RICO” State Societies based their lawsuits on the Racketeer Influenced and Corrupt Organization Act. • Civil – Not criminal – RICO. • Theory – Health plans engaged in fraud and extortion in a common scheme to wrongfully deny payment to physicians. 1 4
Certification of Class a Key Victory • September 26, 2002, Judge Moreno certified the “Provider Track” of the multidistrict litigation as a national class action and ordered discovery to commence on September 30, 2002. • "Here, the Provider Plaintiffs have done more than just allege a common scheme, they have demonstrated facts which support its existence." Slip Opinion at 32. • Defendants appealed the decision. • The United States Court of Appeals for the 11th Circuit upheld Judge Moreno’s decision certifying the class action. On January 10, 2005 the U.S. Supreme Court refused to hear the defendant’s appeal challenging the class action certification. This was a major victory. 1 5
Negotiations With Aetna & CIGNA • All of the plaintiffs, MSSNY and the other State Medical Societies that sued on state law theories and the RICO plaintiffs were included in the negotiations of the Aetna and Cigna settlements. • State Medical Society attorneys and physicians guided our outside counsel in their negotiations with Aetna and CIGNA and participated in drafting settlement language. 1 6
Overview of Settlements • Aetna Agreement dated May 21, 2003 – Final approval by Judge Moreno, October 24, 2003. • CIGNA Agreement dated September 2, 2003 – Final approval by Judge Moreno on April 22, 2004. 1 7
Coverage The settlements include a class of all physicians (over 950,000 physicians, physician groups and physician organizations) who have submitted claims to any of the defendants named in the Complaint (including, Aetna, Anthem, CIGNA, Coventry, HealthNet, PacifiCare, Prudential, United, and Wellpoint). 1 8
Coverage (cont.) • In addition to the Medical Society of the State of New York the settlements also include the following 18 Signatory Medical Societies: Alaska, California, Connecticut, Denton County (TX), El Paso County (CO), Florida, Georgia, Hawaii, Louisiana, Nebraska, New Hampshire, New Jersey, North Carolina, Northern Virginia, South Carolina, Tennessee, Texas and Washington. 1 9
Judge Moreno’s Final Approval Order (Aetna) “… The benefits available directly to the class represent an excellent result….” 1 10
Judge Moreno’s Final Order (cont.) • “The Settlement requires changes and commitments in Aetna’s business practices to eliminate the worst of the improper practices involved in managed care….” • “The settlement creates a substantial fund - $100,000,000 - for physicians to recover some of their damages.” • “The Settlement establishes a foundation dedicated to promoting high-quality healthcare….” 1 11
Effect of Appeals • Judge Moreno’s decision approving the settlement has been appealed. • Aetna will implement injunctive (prospective) relief. • Retrospective relief (monetary payments and funding of the foundation) delayed pending outcome of appeals. 1 12
Settlements Accomplished Goals of Lawsuit • Transparency • Fairness • Coding Problems Fixed 1 13
Components of the Settlements • Retrospective Relief • Prospective Relief • Enforcement 1 14
Aetna Retrospective Relief • $100,000,000 to class members, without any requirement for the submission of documentation. • $20,000,000 to a foundation controlled by the Signatory Medical Societies to the Agreement to create initiatives to improve the quality of healthcare in the country, the Physicians’ Foundation for Health Systems Excellence, Inc. 1 15
CIGNA Retrospective Relief • $30,000,000 to class members who choose not to submit documentation (Category A). • No ceiling on amount for physicians documenting past CIGNA claims (Categories I and II). Minimum of $40,000,000. • Minimum of $15,000,000 to a nonprofit foundation controlled by physicians, the Physicians’ Foundation for Health Systems Innovations, Inc. 1 16
Aetna Prospective Relief in Excess of $300 Million • CIGNA Prospective Relief in Excess of $400 Million • Some Valuations in Excess of $1 Billion 1 17
No Automatic Downcoding Evaluation and management codes will not be automatically downcoded. 1 18
Fairer Payment Rules CPT coding edits must comply with key guidelines contained in the AMA CPT Manual. 1 19
Sample CPT Coding Changes • Modifier 25 separately identified and paid. • Modifier 59 separately identified and paid. • Supervision and interpretation codes separately identified and paid. • Add-on codes eligible for separate treatment. 1 20
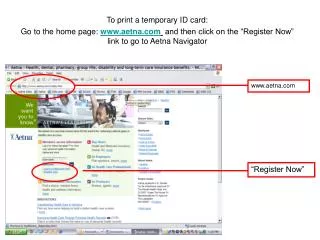
Disclosure of Fee Schedules • Aetna’s physician fee schedules will be available on the Internet by December 31, 2004. • CIGNA will make its fee schedules available to physicians via e-mail. • Fee schedules may be changed only once a year. 1 21
Disclosure of Payment Rules - Aetna • Payment rules will be consistent across all company products by December 31, 2004. • A Web-based pre-adjudication tool will be available on the Aetna Website so that physicians can determine what they will be paid in advance. • Reimbursement edits and claims adjudication logic will be disclosed. 1 22
Disclosure of Payment Rules - CIGNA • A Web-based pre-adjudication tool will be implemented when commercially available. • In the interim, pre-adjudication information available by e-mail. • Reimbursement edits and claims adjudication logic will be disclosed. 1 23
Better Medical Necessity Definition • Patients will be entitled to receive medically necessary care as determined by a physician exercising clinically prudent judgment in accordance with generally accepted standards of medical practice. • Cheaper alternatives are permissible only when they are “at least as likely to produce equivalent therapeutic or diagnostic results.” 1 24
Payment of Vaccines and Vaccine Administration Recommended vaccines and injectibles and the administration of such vaccines and injectibles will be reimbursed. 1 25
Capitation From Date of Enrollment Capitation fees will be paid when the patient chooses a PCP or is assigned to a PCP, retroactive to date of enrollment. 1 26
Participation in Pharmacy Risk Pools Optional Contracting policies will not require the use of pharmacy risk pools. 1 27
Stop-Loss Insurance May Be Purchased Elsewhere Physicians will not be restricted from purchasing stop-loss coverage from other insurers. 1 28
Faster Credentialing New physician group members will be credentialed within 90 days of application, and physicians can submit applications prior to their employment. 1 29
Arbitration Fees Capped Arbitration fees for solo and small group physicians will be capped at $ 1000. 1 30
Gag Clauses Prohibited “Gag” clauses will be prohibited. 1 31
Non-Participating Physicians Protected • Disparaging language will be removed from EOBs. • Rights of non-participating physicians to balance bill patients are protected. 1 32
No HIPAA Mandate • Physicians will not be forced to use electronic transactions or otherwise become HIPAA compliant. 1 33
Physicians’ Input • Physicians' Advisory Committees will be created to address issues of nationwide scope. 1 34
Enforcement of Aetna/CIGNA Settlements • Greatest value of these settlements is injunctive relief. • We can only hold them to their promises with your help. 35 1
Settlements Establish 3 Dispute Resolution Mechanisms • Billing Disputes • Medical Necessity Disputes • Compliance Disputes 1 36
Billing Disputes – Independent Billing Dispute External Review Board • Records submission requirements • Application of coding and payment rules and methodologies to patient specific factual situations • Retained claims – claims in the pipeline on November 6 for services provided prior to that date 1 37
Billing Dispute Resolution Process • Must exhaust internal appeals process – or wait 45 days after submitting all documentation necessary to decide appeal. • Must file no more than 90 days after exhaustion. 1 38
Billing Dispute Resolution Process (cont.) • Must have at least $500 in dispute • Can aggregate claims that are “substantially similar” • Can aggregate claims for 1 year following submission of original dispute. • Must pay filing fee – • $50 minimum + 5% of amount in dispute over $1,000 • Cap of 50% of cost of review. 1 39
Billing Dispute Resolution Process (cont.) • Decision in 30 days of date all documentation received (generally no later than 60 days from original submission of claims satisfying the $500 threshold). • Payment within 15 days of date Aetna receives adverse decision. • PROCESS IS OPTIONAL, but if used, DECISION IS BINDING. 1 40
BURDENSOME RECORDS REQUESTS • Expedited review available if demonstrate by a preponderance of the evidence that the requirement has a significant adverse economic effect which justifies expedited review – otherwise, must exhaust internal appeal. 1 41
WHY MIGHT THIS PROCESS BE BETTER THAN ARBITRATION? • Cases are decided by certified coders and as necessary, professionals in the clinical specialty or area at issue. • Will apply settlement terms, contract terms and “generally accepted medical billing standards” where these are silent. • Settlement terms incorporate better state law where it exists. • Expedited time frame for decisions – generally no more than 60 days. 1 42
GLOBAL IMPACT OF EXTERNAL BILLING DISPUTE RESOLUTION SYSTEM • Aetna will publish a summary of the results of these proceedings annually. • Aetna will refer issues it loses at least 50% of the time in at least 20 proceedings to the Physician Advisory Committee. 1 43
WHAT ALTERNATIVES ARE AVAILABLE? • Any contractual remedies • Arbitration fees are capped at $1000 for physicians in groups of less than 5 • ERISA claimants still have the option of going to federal court. 1 44
Medical Necessity Disputes – generally, state law will be better except for definition of medical necessity. 1 45
Definition of Medical Necessity • Patients are entitled to receive medically necessary care as determined by a physician exercising clinically prudent judgment in accordance with generally accepted standards of medical practice. • Cheaper alternatives are permissible only when they are “at least as likely to produce equivalent therapeutic or diagnostic results.” 1 46
Medical Necessity DisputeResolution Process Overview • Independent external review of determination that services are not medically necessary or are experimental or investigational will be available for physicians by August 6, 2004 or as soon thereafter as practicable. • However, patient pursuit of ERISA suit will trump physician’s rights to external review. 1 47
Medical Necessity Dispute Resolution Process Overview (cont.) • Will meet ERISA timeframes for internal appeals and on physician’s request will consult specialist in same specialty. • Internal process must be exhausted. • Must pay $50 filing fee – or lesser of $250 or external review organization’s fee for matters requiring pre-certification. • Optional – but binding if used. 1 48
Compliance Disputes Any other disputes over enforcement of the Agreement must be: • Submitted on the Compliance Dispute Claim Form • Sent to the Compliance Dispute Facilitator, Julia Stewart, and • Filed within 30 days of the date the Compliance Dispute arose. 1 49
Compliance Disputes (cont.) • Compliance disputes may be filed by Class Members who have been adversely affected by Aetna’s failure to comply with the injunctive relief set forth in the Settlement, or by any Signatory Medical Society on behalf of such a Class Member. 1 50