Download
1 / 67
960 likes | 2.1k Views
URINE FORMATION AND COMPOSITION. Prasetyastuti Dept. of Biochemistry. TOPIC URINE FORMATION NORMAL CONSTITUENTS OF URINE ABNORMAL CONSTITUENTS OF URINE. Kidney. The kidneys’ main function is 1. excretion of water and water-soluble substances . 2. homeostasis

E N D
URINE FORMATION AND COMPOSITION Prasetyastuti Dept. of Biochemistry
TOPIC URINE FORMATION NORMAL CONSTITUENTS OF URINE ABNORMAL CONSTITUENTS OF URINE
Kidney The kidneys’ main function is 1. excretion of water and water-soluble substances. 2. homeostasis This is closely associated with their role in regulating the body’s electrolyte and acid– base balance
Both excretion and homeostasis are subject to hormonal control. 3. involved in synthesizing several hormones 4. play a role in the intermediary metabolism, particularly in amino acid degradation and gluconeogenesis
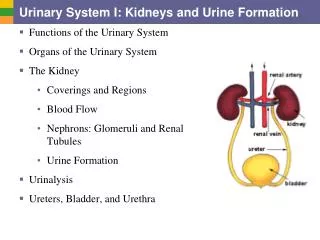
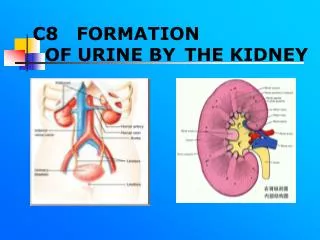
Urine formation - The functional unit of the kidney is the nephron. - It is made up of * the Malpighian bodies or renal corpuscles (consisting of Bowman’s capsules and the glomerulus), * the proximal tubule, * Henle’s loop, and *the distal tubule, --- which passes into a collecting duct.
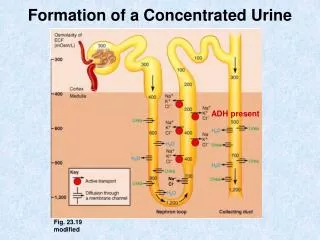
The human kidney contains around one million nephrons. The nephrons form urine in the following three phases. 1. Ultrafiltration. Ultrafiltration of the blood plasma in the glomerulus gives rise to primary urine, which is isotonic with plasma.
2. Resorption. All low-molecular weight plasma components enter the primary urine via glomerular filtration. Most of these are transported back into the blood by resorption, to prevent losses of valuable metabolites and electrolytes.
3. Secretion. Some excretable substances are released into the urine by active transport in the renal tubules. These substances include H+ and K+ ions, urea, and creatinine, as well as drugs such as penicillin.
The pores in the glomerular basal membrane, which are made up of type IV collagen, have an effective mean diameter of 2.9 nm. This allows all plasma components with molecular mass of up to about 15 kDa to pass through unhindered. > 65 kDa, they are completely unable to enter the primary urine.
In the proximal tubule, organic metabolites (e. g., glucose and other sugars, amino acids, lactate, and ketone bodies) are recovered by secondary active transport There are several group-specific transport systems for resorbing amino acids, with which hereditary diseases can be associated (e. g., cystinuria, glycinuria, and Hartnup’s disease).
In alkaline urine a turbidity - precipitation of CaPO4 • Strongly acid urine precipitates uric acid salts -- pink color E Odor - Fresh urine is normally aromatic but the odor may be modified by substances in the diet such as asparagus (methyl mercaptan odor) In ketosis -- acetone odor
Urine • Urine: • Is an ultrafiltrate of plasma from which glucose, amino acids, water and other substances essential to body metabolism have been reabsorbed. • Urine carries waste products and excess water out of the body. Urine consists of: Inorganic: Cl-, Na, K. trace amounts of: sulfate, HCO3 etc.) (96%) water (2%) Urea: (half) (2%) Other compounds (4%) dissolved solids: Organic:creatinine uric acid
Urine Characteristics A. Volume • - Adults produce from 750ml-2500ml / 24h, with the average of about 1.5L per person. around 95% of which consists of water. - The volume and composition of urine are subject to wide variation and depend on - food intake, - bodyweight, - Age - sex, and
- living conditions such as temperature,humidity, physical activity, and health status. • Nitrogenous end product and coffee, tea, and alcoholic beverages have a diuretic effect B. Specific Gravity • 1.003- 1.030 and varies according to concentration of solutes in the urine • The total solids in the urine 50g/1200ml /d
C. Reaction - the urine normally acid, with a pH < 6 ( 4.7-8.0) • > 250 ml of 0.1 N acid, 25 mEq H ion are excreted daily - The urine is acid when - the protein intake is high, because excess phosphate & sulfate are produce in the catabolism of protein • in acidosis • in fevers
The urine become alkaline - on standing because of convertion of urea to ammonia and loss of CO2 to air - in alkalosis (after excessive vomiting, after meals due to H+ secretion in the stomach ) D. Color - Pale yellow or amber - Varies with quantity and concentration of urine voided
- The chief pigment is urohrome, but small quantities of urobilin and hematoporphyrin - in fever -- dark yellow or brownish - In liver disease -- green, brown or deep yellow - Blood or Hb - smoky to red color • Met Hb & homogenticid acid - dark brown • Methylene blue - green • Cascara & cathartics - brown color
Amber yellow Urochrome(derivative of urobilin, produce from bilirubin degradation, is pigment found in normal urine). • Colorless due toreduced concentration. • Silver or milky appearance Pus, bacteria or epithelial cells • Reddish brown Blood (Hemoglobin). • Yellow foam Bile or medications. • Orange, green, blue or red medications. • Vitamin B supplements can turn urine bright yellow.
HCO3–, Na+, phophate, and sulfate are also resorbed by ATP-dependent (active) mechanisms in the proximal tubule The later sections of the nephron mainly serve for additional water recovery and regulated resorption of Na+ and Cl– These processes are controlled by hormones (aldosterone, vasopressin).
Clearance. Renal clearance is used as a quantitative measure of renal function. It is defined as the plasma volume which contains the amount of the substance which is excreted in the urine in 1 minute Inulin, a fructose polysaccharide with a mass of 6 kDa that is neither actively excreted nor resorbed but is freely filtered, has a clearance of 120mL /min in healthy individuals
Concentrating urine and transporting it through membranes are processes that require large amounts of energy. The kidneys therefore have very high energy demands. In the proximal tubule, the ATP needed is obtained from oxidative metabolism of fatty acids, ketone bodies, and several amino acids. To a lesser extent, lactate, glycerol, and citric acid are also used.
In the distal tubule an Henle’s loop, glucose is the main substrate for the energy metabolism. The endothelial cells in the proximal tubule are also capable of gluconeogenesis. Enzymes for peptide degradation and the amino acid metabolism occur in the kidneys at high levels of activity (e. g., amino acid oxidases, amine oxidases, glutaminase).
NORMAL CONSTITUENTS OF URINE A. UREA - Is the principle end product of protein metabolism in mammals • Its excretion is directly related to the protein intake • Normally it comprises 80-90% of the total urinary nitrogen - On low protein diet this is less, because certain other nitrogenous constituents tend to remain relatively unaffected by diet
Urea excretion is increased when • Protein catabolism is increased - in fever, diabetes, excess adrenocortical activity Urea excretion is decreased in • The last stages of fatal liver disease - Acidosis ( nitrogen --urea -- amonia)
B. AMMONIA • Maybe present - in inorganic combination or - in the free state • Normally there is very little • About 2,5- 4,5 % of the total nitrogen of the urine is eliminated as ammonia ± 0,7 g/day • Increased excretion in acidosis • Decreased excretion in ketosis - To be related to the acid-base balance in the body
C. CREATININE Anhydride of creatine (methylguanidino acetic acid) • Is the product of the breakdown of creatine • The creatinine coefficient is the ratio between the amount of creatinine excreted in 24 hours and the body weight in kg • -- 20-26 mg/kg/day : normal men (1-1,8 g/d) • -- 14- 22 mg/kg/day : normal women - Creatinine excretion is decreased in many patologic states • Creatinine is measured colorimetrically by Jaffe reaction - red color
D. CREATINE • in children > adults • Excretion - men 6% total creatinine output(60-150 mg/d) - women ( 2-2.5 times normal men ) - is increased in - pregnancy, starvation, fever, impaired carbohydrate metab, hyperthyroidism , certain myopathies infection, carcinoma of the liver - is decreased in hypothyroidism
E. URIC ACID • The most important end product of the oxidation of purine in the body • Is derived from - dietary nucleoprotein - breakdown of cellular nucleoprotein in the body • The normal in urine : 0,5 – 1,0 g/24 h
On a purine –free diet : 0,1-0,5 g/d • On high purine diet :2 g/d • Uric acid acts as a weak dibasic acid and forms two classes of salt, neutral and acid - In urine in the form of urates and upon acidifying the liquid the uric acid is liberated and deposits in crystalline form
The output is increased in • leukemia, severe liver disease, various stages of gout • After a large dose of aspirin excretion of uric acid raise as much as 25% in 24 hours • Analysis for uric acid by - Folin test : not specific - uricase enzyme : uric acid - allantoin
F. AMINO ACIDS • In adults : 0,4-1,0 g / 24 h are excreted • The full-term infant at birth : 3 mg/pound bw declines gradually up to the age of 6 months • When it reaches a value of 1 mg/lb maintained through chilhood - Premature infants : 10 times the full-term
Renal thresholds are quite high - very small amount in urine • The excreted is increased in - terminal liver disease - certain types of poisoning(CHCL3,CCL4) - cystinuria ( arg,cys,lys, orn) all other aa excreted remain normal - thypoid - acidosis
G. ALLANTOINIs derived from partial oxidation of uric acid by uricase Principal end product of purine catabolism in other subprimate mammals - Normal excretion : 5 – 15 mg/day H. CHLORIDE • Are mainly excreted as NaCl • Output varies considerably with intake • The daily output is about 10-15 g - Excessive loss of NaCl : muscular cramps
I SULFATES • Is derived from protein because of the presence of the sulfur containing amino acid (methionine and cystein) in the protein molecule. The total urine sulfur is partitioned into 1.inorganic (sulfate) sulfur (SO3) Urin + BaCl2 -- sulfur precipitated
proportionate to the ingested protein with a ratio 5:1 between urine nitrogen and inorganic sulfate 2. Ethereal sulfur (conjugates sulfate) - about 10% of the total sulfur - ethereal sulfur and organic combination of sulfur excreted in the urine phenol & cresol sulfuric acid indoxyl & skatoxyl sulfuric acid
3. Neutral sulfur • Is the sulfur which is incompletely oxidized such as that which is contained in cystein, taurine, thiocyanate, or sulfides • Neutral sulfur : total sulfur – ( inorganic + ethereal sulfur)
J. PHOSPHATES • The urine phosphate are combination of Na & K phosphate Ca & Mg phosphate : precipitated in alkaline urine • Output increase in - osteomalacia, renal tubular rickets - hyperparathyroidism - periostosis
Output decrease in - hypoparathyroidism. - fibrile affections ( acute infection disease) • Total output - inorganic phosphate : 1.1 g/ 24 h - organic phosphate : 1-4% of the total
K. OXALATES- primer hyperoxaluria (inherited metabolic disease ---- large quantities in urine - about 20-50 mg/d L. MINERAL ( sodium, potasium, calcium, magnesium) Sodium content varies considerably with intake & physiologic requirements -
The excretions are controlled by the activity of the adrenal cortex - Excreted 3-5 g/24 h • The ratio of K and Na is generally about 3:5 Calcium • The daily output 0.1-0.3 g/d • High excretion in osteomalacia
Magnesium- The daily output 0.05-0.2 g/d- ≥ 65% eliminated by feces, the remainder passes out in the kidneys Potassium Urine potassium increase when - intake is increased - the presence of excessive tissue catab - in alkalosis
- are controlled by the activity of the adrenal cortex - is excreted 1-3 g/24 h M. VITAMIN, HORMON, AND ENZYME • Can be detected in small quantities - The urinary content is often of diagnostic importance
ABNORMAL CONSTITUENTS OF THE URINE A. PROTEIN • Proteinuria (albuminuria) is the presence of albumin and globulin in the urine in abnormal concentrations Normally < 30-200 mg /d are excreted
1. physiologic proteinuria, less than 0.5% protein in present - after severe exercise - after a high-protein meal - as a result of some temporary impairment in renal circulation when a person stands erect - in 30-35% of the cases, pregnancy is accompanied by proteinuria
2. pathologic proteinuria classified as a. prerenal: when the primary causes are factors operating before the kidney is reached, although the kidney may also be involved
b. renal : when the lesion is intrinsic to the kidney c. post renal : when the proteinuria is due to inflamma tion in the lower urinary tract • In glomerulonephritis proteinuria is marked during the generative phase
The lowest excretion of albumin is during the latent phase and may increase terminally In nephrotic syndrome accompanied by edema & low concentration of serum albumin
Nephrosclerosis : vascular form of renal disease - is related to arterial hypertension - with the increasing severity of the renal lesion. - is generally less than that in glomerulone phritis Poisoning of the renal tubule by heavy metals mercury, arsenic, bismuth
3. Albumin heating the urine centrifuging -- supernatan + acetic acid white cloud /ppt - protein is present quantitative , with TCA --- colorimetrically or kjeldahl analysis 4. Bence Jones protein • Peculiar proteins are light chain fragments of globulins which occur in the urine - commonly in multiple myeloma