Download
1 / 16
160 likes | 250 Views
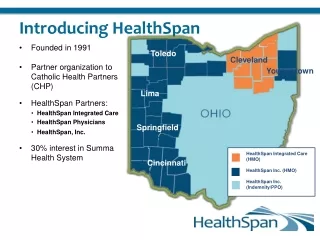
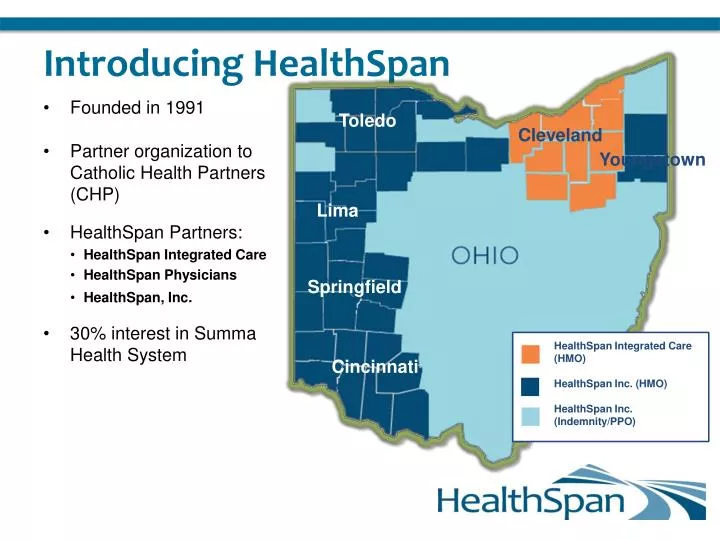
Introducing HealthSpan. Founded in 1991 Partner organization to Catholic Health Partners (CHP) HealthSpan Partners: HealthSpan Integrated Care HealthSpan Physicians HealthSpan, Inc. 30% interest in Summa Health System. Toledo. Cleveland. Youngstown. Lima. Springfield.

E N D
Introducing HealthSpan • Founded in 1991 • Partner organization to Catholic Health Partners (CHP) • HealthSpan Partners: • HealthSpan Integrated Care • HealthSpan Physicians • HealthSpan, Inc. • 30% interest in Summa Health System Toledo Cleveland Youngstown Lima Springfield HealthSpan Integrated Care (HMO) HealthSpan Inc. (HMO) HealthSpan Inc. (Indemnity/PPO) Cincinnati
The Changing Healthcare Landscape Presented by: Dr. Nick Dreher, Medical Director
Payment Reform Average US Salary vs. Health Insurance Premium • From 1999 – 2009, salaries have increased 38% while premiums have increased 131% If other prices grew as quickly as healthcare costs since 1945 • Dozen eggs would cost $55 • Gallon of milk would cost $48 • Dozen oranges would cost $134 Institute of Medicine, 2011
Affordable Care Act and Healthcare Reform Current: Fee For Service New Model: Reward Quality Outcomes and Stewardship of Resources
Uncoordinated care Over-loaded schedule Physician and practice-centric Arbitrary quality improvement projects Lack of clear leadership and support Extreme Makeover Home Edition Team-based approach Open access Patient engagement and empowerment Data-directed quality improvement Engaged leadership
What Is the Solution? TRANSFORMATION • beyond transaction • through technology • to manage shared risk • by connecting • for our patients VALUE DRIVEN CARE
How Do We Improve Care and Manage Costs? Patient-Centered Medical Home (PCMH) is one way
Care Coordination: What Is It? • The goals of coordinated care • Ensure that patients, especially the chronically ill, get the right care at the right time • While avoiding unnecessary duplication of services AND preventing medical errors VALUE for the Patient = QUALITY/COST
Care Coordination • AIM • Effectively identify, manage and track results of PCMH’s high risk patient population through care coordination, patient coaching and education, application of Evidence Based Medicine, and population data analysis and reporting • Interventions • Embed Care Coordination Teams in Primary Care offices, identify high-risk patients and provide high touch to these patients
What Are the Components of the ACO? A group of providers willing and capable of accepting accountability for the total cost and quality of care for a defined population. • Core Components: • People Centered Foundation • Health Home • High-Value Network • Population Health Data Mgmt • ACO Leadership • Payer Partnerships • Payer Partners • Insurers • Employers • States • CMS
Tying It All Together Integrated elements of a successful ACO • Improved clinical outcomes and patient satisfactionlinked to • Care Coordination embedded in • Patient Centered Medical Homespracticing • Improvement Science Methodologies that support • Population Health Management using • Data Analytics across a Clinically Integrated Organization
Where Does Wellness Fit In?(To Date, Wellness has not Proven Sustainable Outcome Improvements for Large Populations.) • Interlinking Electronic Medical Record with Wellness Platform. • Physician participation in Wellness goals and monitoring. • Physician based treatment protocol for behaviors related to morbidity, (addiction, obesity, etc…)