Download
1 / 16
160 likes | 168 Views
HealthSpan, a partner organization to Catholic Health Partners, offers integrated care solutions for improved patient outcomes and cost management. Learn about population health management, care coordination, and accountable care organizations in the changing healthcare landscape.

E N D
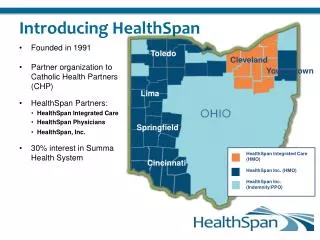
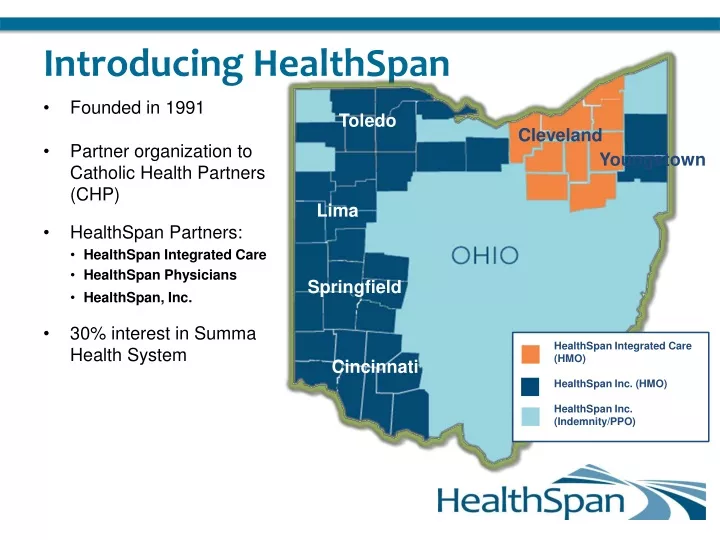
Introducing HealthSpan • Founded in 1991 • Partner organization to Catholic Health Partners (CHP) • HealthSpan Partners: • HealthSpan Integrated Care • HealthSpan Physicians • HealthSpan, Inc. • 30% interest in Summa Health System Toledo Cleveland Youngstown Lima Springfield HealthSpan Integrated Care (HMO) HealthSpan Inc. (HMO) HealthSpan Inc. (Indemnity/PPO) Cincinnati
The Changing Healthcare Landscape Presented by: Dr. Nick Dreher, Medical Director
Payment Reform Average US Salary vs. Health Insurance Premium • From 1999 – 2009, salaries have increased 38% while premiums have increased 131% If other prices grew as quickly as healthcare costs since 1945 • Dozen eggs would cost $55 • Gallon of milk would cost $48 • Dozen oranges would cost $134 Institute of Medicine, 2011
Affordable Care Act and Healthcare Reform Current: Fee For Service New Model: Reward Quality Outcomes and Stewardship of Resources
Uncoordinated care Over-loaded schedule Physician and practice-centric Arbitrary quality improvement projects Lack of clear leadership and support Extreme Makeover Home Edition Team-based approach Open access Patient engagement and empowerment Data-directed quality improvement Engaged leadership
What Is the Solution? TRANSFORMATION • beyond transaction • through technology • to manage shared risk • by connecting • for our patients VALUE DRIVEN CARE
How Do We Improve Care and Manage Costs? Patient-Centered Medical Home (PCMH) is one way
Care Coordination: What Is It? • The goals of coordinated care • Ensure that patients, especially the chronically ill, get the right care at the right time • While avoiding unnecessary duplication of services AND preventing medical errors VALUE for the Patient = QUALITY/COST
Care Coordination • AIM • Effectively identify, manage and track results of PCMH’s high risk patient population through care coordination, patient coaching and education, application of Evidence Based Medicine, and population data analysis and reporting • Interventions • Embed Care Coordination Teams in Primary Care offices, identify high-risk patients and provide high touch to these patients
What Are the Components of the ACO? A group of providers willing and capable of accepting accountability for the total cost and quality of care for a defined population. • Core Components: • People Centered Foundation • Health Home • High-Value Network • Population Health Data Mgmt • ACO Leadership • Payer Partnerships • Payer Partners • Insurers • Employers • States • CMS
Tying It All Together Integrated elements of a successful ACO • Improved clinical outcomes and patient satisfactionlinked to • Care Coordination embedded in • Patient Centered Medical Homespracticing • Improvement Science Methodologies that support • Population Health Management using • Data Analytics across a Clinically Integrated Organization
Where Does Wellness Fit In?(To Date, Wellness has not Proven Sustainable Outcome Improvements for Large Populations.) • Interlinking Electronic Medical Record with Wellness Platform. • Physician participation in Wellness goals and monitoring. • Physician based treatment protocol for behaviors related to morbidity, (addiction, obesity, etc…)