Download
1 / 13
130 likes | 245 Views
Requesting Healthcare Expense Payments. Through the Friend of the Court. Prior to contacting the FOC. Check your court order to verify that it requires the other party to pay a portion of health care expenses.

E N D
Requesting Healthcare Expense Payments Through the Friend of the Court
Prior to contacting the FOC • Check your court order to verify that it requires the other party to pay a portion of health care expenses. • Submit your request for payment to the other party within 28 days of either the date insurance has paid on the expenses or the date the insurance denies payment.
Prior to contacting the FOC • For each expense that you list on the first notice: • Include the date insurance paid on the expense (or), • Include date insurance denied payment (or), • Include date of service for the expense when there is no insurance available.
Response from the other party • You and the other party may reach an agreement concerning the expenses. • Agreement must be in writing. • Agreement must state the total to be paid and the payment schedule. • Both parties must sign the agreement.
Attach copies of Bills and Insurance notifications The “Request for Healthcare Expense Payment” form • Obtain from the Friend of the Court OR from http://courts.michigan.gov/scao/courtforms/domesticrelations/ drindex.htm • Use this form to submit to the other party. • Wait 28 days for response from the other party.
Contacting the FOC • Present bill and white copy of the first notice that you sent to the other party- to the FOC within: • One year after the expense was incurred - OR- • 6 mos. after insurer’s final denial of coverage for the expense (was incurred) - OR - • 6 mos. After a default in a repayment agreement between you and the other party per the terms agreed upon
When default occurs • You have not received an agreement for payment. • You have waited 28 days from the mailing of the first notice to the other party • The other party has missed an agreed upon payment within the payment schedule.
2nd FORM The Complaint For Enforcement of Healthcare Expense Payment Contacting the FOC • You will need to fill out a SECOND form to request enforcement.
The second notice • Complete the “Complaint for Enforcement of Healthcare Expense Payment” form • Attach supporting bills and receipts for each expense you list. • Attach copy of all insurance notifications for each expense you list.
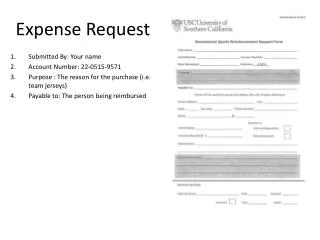
The Complaint 02-012345-DM JOHN DOE JANE DOE Complete JOHN DOE 123 MAIN ST. ADRIAN, MI 49221
The Complaint Complete Complete Complete Date & Sign
Medical Enforcement • Your Enforcement Officer is your primary contact for Medical Enforcement through the FOC. • The FOC fax line is: 264-4765.
Requesting Healthcare Expense Payments Thank you. Please contact your Enforcement Officer if you need further information.