Download
1 / 28
280 likes | 624 Views
Doses of anti-TB drugs for children: promoting the development of improved recommendations based on pharmacokinetic studies in children. HS Schaaf, PR Donald Paediatrics and Child Health Tygerberg Children’s Hospital Stellenbosch University Cape Town South Africa.

E N D
Doses of anti-TB drugs for children:promoting the development of improved recommendations based on pharmacokinetic studies in children HS Schaaf, PR Donald Paediatrics and Child Health Tygerberg Children’s Hospital Stellenbosch University Cape Town South Africa
Reis FJC, Bedran MBM, Moura JAR, Assis I, Rodrigues MESM. Six-month isoniazid-rifampin treatment for pulmonary tuberculosis in children. Am Rev Respir Dis 1990; 142: 996-999 “It is very difficult to assess the outcome and efficacy of any regimen for treatment of tuberculosis in children because they rarely have positive sputum and gastric washings and the best criteria would be clinical findings, such as weight gain and radiologic follow-up studies.”
Children are not just small adults! Response to tuberculosis infection • Differing spectrum of disease (EPTB) • Disease vs. Infection • Relatively benign course of most tuberculosis infections
Children are not just small adults! Non-linear changes in body composition • Body weight: doubles by 5-months, triples by a year. • Body length: increases by 50% by 1-year • Body surface area: doubles by 1-year • Total body water: 85% in premature neonate 70% in full term infant 55% in an adult • Protein binding reaches adult levels at approximately 1-year
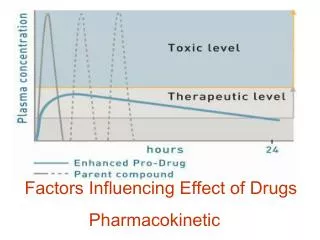
Similar to adults, a relationship between what the body does with a drug (pharmacokinetics) and what the drug does to the body (pharmacodynamics) is present in children • It is mainly the pharmacokinetics that change during childhood, but pharmacodynamics is important, as some drug adverse events may mainly present in children
Children are not just small adults! Developmental differences occur in all aspects of drug metabolism • Absorption (gastric pH, gastric emptying, first-pass metabolism in stomach, bowel or liver) • Distribution (changes in body composition, protein or tissue binding) • Metabolism (complicated, many enzymes involved) • Excretion (liver and kidney are several fold greater relative to body weight in children compared to adults) (McCarver DG. Pediatrics 2004; 113: 969-972)
Anti-TB drug levels in children • WHO recently published a literature review on EMB by Peter Donald. This showed:“Peak serum EMB concentrations in both children and adults increase in relation to dose, but are significantly lower in children than adults receiving the same mg/kg body weight dose.” It was recommended that the dose for children should be 20 mg/kg (15-25 mg/kg)
The data used in figure are derived from a number of papers. The two lines are Adults: y=0.1602*Dose and Children: y=0.0906*Dose. The standard errors of the two slope coefficients are respectively, 0.005833 and 0.009080. The difference between the slopes is clearly significant
Schaaf HS et al. Isoniazid pharmacokinetics in children treated for respiratory tuberculosis. (Arch Dis Child 2005;90:614-618 • INH serum concentrations determined at 2-, 3-, 4- and 5-hours after dosing with INH 10 mg/kg bodyweight in 64 children median age 3.8 years was - • compared to serum concentrations of INH in 60 adult patients also receiving 10 mg/kg bodyweight INH. (Parkin et al Am J Respir Crit Care Med 1997; 155: 1717-1722)
AUC and 2-hour serum concentrations of INH in adults and children after an INH dose of 10 mg/kg body weight Genotype AUC (mg/l/hr) 2 hr Conc (µg/ml) Adults Child AdultsChild SS 24.918.36 10.948.60 FS 15.38 8.25 8.705.13 FF 8.14 5.37 6.033.94
2-hr INH concentration vs. dose. The 2-hour INH serum concentration associated with the EBA90 is 2.19 µg/ml
INH study results • Considerable differences in exposure to INH between slow, intermediate and fast acetylators – in adults and children • Younger children eliminate INH faster than older children. In a trimodal model of INH elimination there is a significant age related decline in the first order elimination rate constant (k, h-1) with age in all three groups
INH study results • Exposure of children to INH, as reflected by k h-1, AUC(2-5 hrs after dosing) and INH concentration at different time intervals after dosing, is significantly less than that of a group of adults drawn from the same population and receiving the same mg/kg body weight dose of INH • In this population, intermediate + fast acetylators are in the majority (approx. 60%+)
INH study results • These findings, taking into account the NAT2 genotype, confirm that younger children eliminate INH faster than older children, and children, as a group, faster than adults • WHO and IUATLD currently recommend 5 mg/kg (4-6) INH for children and adults. However, AAP recommends an INH dose of 10-15 mg/kg/dose
Median rifampicin concentrations in adults (red) and children (pink) established on first-line treatment sampling 1.5, 3, 4 and 6 hours after dosing with standard daily doses
Peak rifampicin serum concentrations in adults (A) and children (C). (Kruskall-Wallis P=0.562)
Rifampicin area under the curve (AUC) in adults (A) and children (C). (Kruskall-Wallis P=0.009)
Rifampicin half-life in adults (A) and children (C). (Kruskall-Wallis P=0.0001)
Rifampicin and Rifapentine • Rifampicin results shown are provisional results from a study in Cape Town (PR Donald, H McIlleron, et al.) • Pharmacokinetics of Rifapentine in children: (MJ Blake et al. PIDJ 2006;25:405-408)“Given a comparable weight-normalized dose, rifapentine exposure estimates are lower in children than those reported in adults, suggesting that a larger weight-normalized (i.e. mg/kg) dose of rifapentine is needed in children”
Pyrazinamide • Incomplete or delayed absorption was more common in children than in adults • Median volume of distribution (L/kg) was 32% larger in children, and median clearance (L/hr/kg) was 106% larger in children, with a resultant median half-life 43% shorter in children M Zhu et al. Population pharmacokinetic modeling of pyrazinamide in children and adults with tuberculosis. Pharmacotherapy 2002;22:686-695
Pyrazinamide • Graham et al. found poor absorption of PZA in Malawian children and that younger children (<5 yrs) reached significantly lower serum PZA concentrations than older children • In almost all cases , the Cmax failed to reach the MIC for M. tuberculosis
How then best to assess an antituberculosis agent for a paediatric indication? Perhaps? • Accept evidence of efficacy from adult studies BUT • Evaluate differences in pharmacokinetics and pharmacodynamics before making a recommendation for dose in children
“The true maximum dose is the highest dose that a patient can tolerate, hopefully while achieving the desired therapeutic response” Charles A Peloquin (1998)
Way Forward? • Need more pharmacokinetic and pharmacodynamic anti-TB agent studies in children • Reviews of existing data not only on EMB and INH, but also on other first-line anti-TB drugs (RMP, PZA)