Download
1 / 55
560 likes | 1.31k Views
Step into the void: Vestibular deficits in children with hearing loss. Genevieve DelRosario, MHS, PA-C University of Kansas Medical Center Kansas City, Kansas. Objectives. Review vestibular physiology and pathophysiology Discuss the evaluation of a child’s vestibular status

E N D
Step into the void: Vestibular deficits in children with hearing loss Genevieve DelRosario, MHS, PA-C University of Kansas Medical Center Kansas City, Kansas
Objectives • Review vestibular physiology and pathophysiology • Discuss the evaluation of a child’s vestibular status • Be able to develop a plan for a child with vestibular dysfunction
Vestibular system: A “sixth sense” • Allows us to know where we are in space • Orient selves with respect to gravity • Unifying system that allows us to process information from other senses
Where does our sense of balance come from? • Eyes • Sensors in joints, muscles, and feet • Balance organs in the ears
Vestibular system • Vestibular ocular system • Responsible for visual stabilization • Vestibular spinal system • Maintains orientation of the body in space • Contributes to the postural tone necessary for the acquisition of motor development milestones
Development of the vestibular system • Very old in evolutionary terms • Emerges early in embryonic development • Prior to vision and hearing • Peak developmental time is 6-12 months • Continues development through childhood
http://www.qmw.ac.uk/~ugha014/vestibular%20stuff/vestibular3.htmlhttp://www.qmw.ac.uk/~ugha014/vestibular%20stuff/vestibular3.html
http://www.qmw.ac.uk/~ugha014/vestibular%20stuff/vestibular3.htmlhttp://www.qmw.ac.uk/~ugha014/vestibular%20stuff/vestibular3.html
Prevalence of vestibular dysfunction* • 20-70% of children with hearing loss • Higher in profound HL vs. severe • Continuum of severity • Mild loss to vestibular areflexia * Angeli 2003.
What happens in deaf/HOH children? • Semicircular canals may be absent • Hair cells may be damaged, absent, or reduced • Nerve damage • Enlarged vestibular aqueduct • ???
Better or worse? • In general, balance improves as you age • Vestibular maturation continues through adolescence • Vestibular deficits in deaf/HOH may worsen • Small study showed progressive gross motor and balance difficulties1 • Contradicted by other studies2 1. Rine et al 2000. 2. Siegel et al 1991.
How does it feel? http://www.theraider.net/films/crusade/making_4_postproduction.php
How does it feel (adult perspective)? • Headache • Feeling of ear fullness • Imbalance to the point of being unable to walk • Bouncing and blurring of vision (oscillopsia) • Inability to tolerate head movement • Difficulty walking in the dark • Feel unsteady; actual unsteadiness while moving • Lightheadedness • Severe fatigue In severe cases, symptoms such as oscillopsia and problems with walking in the dark are not going to go away. www.vestibular.org
Oscillopia www.dizziness-and-balance.com
Signs of poor vestibular function • Low muscle tone • Delayed loss of primitive reflexes • Delayed gross motor milestones • Developmental delays • Seizures • Nystagmus • Easy fatiguability • Reflux
Signs of poor vestibular function • Low muscle tone • Delay in holding head up • “Snuggly” baby • “Floppy baby” • Arching of back
Signs of poor vestibular function Delayed disappearance of newborn reflexes • Moro • ATNR: Asymmetric tonic next response • Usually disappear by 6-7 months http://www.frisbee.li/webobtimierte-bilder/abb1.jpg
Signs of poor vestibular function • Delayed motor milestones • Average deaf child walks at 14 months • Average child with Usher’s Type 1 walks at 20 mos • Delays sitting, crawling, climbing steps, hopping… • Speech delays
What do older children look like? • Clumsy • Unable to walk on a balance beam • Problems standing with feet together and eyes closed (Romberg test) • Love spinning, merry-go-rounds, water activities
Weak VOR • Challenges with reading • Gaze instability causes problems with acuity* Braswell & Rine 2006. www.fotosearch.com
My deaf child is a late walker…does that mean she has vestibular problems?
No, but it’s a red flag!Consider also: • Vision problems • Global developmental delay • Autistic spectrum disorder • Just taking her sweet time!
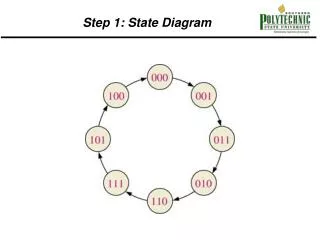
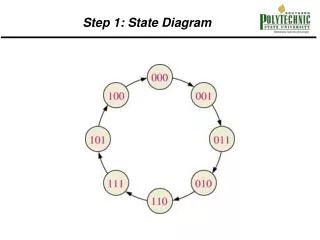
Tests of vestibular function • Eye tracking tests • Positional/positioning tests • Dix-Hallpike • Supine • Rotational tests • Rotary chair testing is gold standard
Causes of poor vestibular function • Postnatal acquired cases • Meningitis • Labyrinthitis • Some forms of syndromic deafness • Labyrinthine dysplasia • Ototoxicity
Conditions associated with CHL and poor balance • Usher’s Syndrome (Type 1) • Waardenburg Syndrome • Pendred syndrome • ESPN mutation • CHARGE Syndrome • Brachio-oto-renal syndrome • ….and more!
Usher’s Syndrome • Autosomal recessive syndrome • Hearing loss, vision loss, and variable vestibular dysfunction • Visual loss is due to retinitis pigmentosa • Three types
Usher’s syndrome • Type 1 • Born profoundly deaf • Vision loss typically noted by age 10 • Absent vestibular function • 3-6/100,000 individuals • ~ 5% of deaf individuals • Type 2 • Moderate to severe hearing loss • Vision loss typically begins after teen years • Normal vestibular function • Type 3 • Born with normal hearing, varying rate of loss • Night blindness during puberty • Normal or near-normal vestibular function
Retinitis pigmentosa <> <>
Retinitis pigmentosa http://www.blindness.org/content.asp?id=45
Waardenburg Syndrome http://www.werathah.com/deafness/waardenburg.htm
Pendred Syndrome http://www.bmm.charite.de/rueckschau/ribeiro/ribeiro.htm
CHARGE Syndrome • Coloboma of the eye • Heart defects • Atresia of the choanae • Retardation of growth and/or development • Genital and/or urinary abnormalities • Ear abnormalities and deafness www.charrgesydnrome.org
Brachio-oto-renal syndrome • Autosomal dominant • Malformation of ear • cochlear hypoplasia • enlargement of the cochlear and vestibular aqueducts • hypoplasia of the lateral semicircular canal • Hearing loss • Malformations of kidney
ESPN Mutation • Autosomal recessive mutation • Mapped to chromosome 1p36.3
Environmental causes • Aminoglycoside antibiotics • Gentamicin, streptomycin, kanamycin, tobramycin, neomycin, amikacin, netilmicin, dihydrostreptomycin, and ribostamycin. • Anti-neoplastics • Cisplatin, carboplatin • Environmental chemicals • Butyl nitrite, mercury, carbon disulfide, styrene, carbon monoxide, tin, hexane, toluene, lead, trichloroethylene, manganese, xylene, mercury • Loop diuretics • Bumetanide, ethacrynic acid, furosemide, and torsemide. • Aspirin and quinine products • Infections www.vestibular.org
Vestibular effects of cochlear implantation • Rare cause of permanent damage • Common cause of transient damage • 20% in one series1 • Anecdotal evidence for improvement • Hearing with CI does not make a difference2 1: Vilbert et al 2001. 2. Suarez et all 2007.
I think the child I am treating may have vestibular problems. Now what?
Evaluation • CT of temporal bone • Vestibular testing (if possible) • Physical, occupational, ? cognitive therapies • Genetic appointment • Strongly consider testing for Usher’s mutations • Vision evaluation • ?ERG
Therapeutic goals • Enhance existing vestibular capabilities • Strengthen compensatory mechanisms http://www.tradecards.com/articles/thread/thread11.html
Compensatory mechanisms • Proprioceptive input • Walking barefoot or soft soled shoes • Visual input • Other sensory systems
Therapies for children with poor vestibular systems • Swinging • Rocking • Bouncing/jumping • Dancing • Skipping • Running • Hopping • Jumping rope • Rough and tumble play http://static.flickr.com/49/131593782_00522c7610_m.jpg
Other interventions • May wear weighted vests, leg weights, etc • Consider orthopedic shoes • OR soft soled shoes • Offer sensory activities • May need extra time to process information www.bright-start.com
Does treatment make a difference? • Motor development improved post treatment1 • Therapy three times weekly for 12 weeks • Visual and somatosensory function, balance training • Significant improvement in motor development • Insignificant improvement in posturography • May improve gaze stability2 • Preliminary study of two individuals 1. Rine et al 2004. 2. Braswell and Rine 2006.
Treatment challenges • Lack of data • Especially true for infants and toddlers • Different causes of balance problems
Cautions with poor vestibular function • Where visual and proprioceptive information is unreliable • Eg, swimming in the dark • Problems with depth perception • Tunnel vision can cause problems • Worse in unfamiliar places
Implications for future research • Vestibular hypofunction in infancy and early childhood poorly understood • Need for research on both function and treatment