Download
1 / 15
210 likes | 1.2k Views
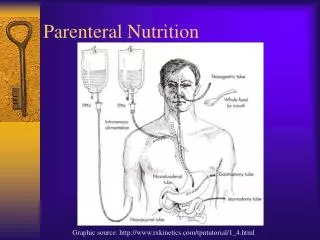
Audit on Total Parenteral Nutrition in Neonates Dr I Ebrahim - SHO in Paediatrics - JPH. Marker for quality of care Audit to ensure current practice is in accordance with hospital TPN guideline. INDICATIONS FOR TPN Absolute Non patent G.I. Tract prior to surgery Post gastrointestinal surgery

E N D
Audit on Total Parenteral Nutrition in NeonatesDr I Ebrahim - SHO in Paediatrics - JPH • Marker for quality of care • Audit to ensure current practice is in accordance with hospital TPN guideline
INDICATIONS FOR TPN Absolute • Non patent G.I. Tract prior to surgery • Post gastrointestinal surgery • Short Gut Syndrome • Non functioning Gut - NEC Possible indicators • Gestation age < 30/40 • Weight < 1500gm • Ventilated > 48 hours • On conservative treatment for NEC • Absent/reversed end diastolic flow on doppler
CONSTITUENTS OF TPN Carbohydrate: Major source of energy Protein sparing effect Disadvantages: Hyperglycaemia Cannot be infused above a certain rate Lipids: Provide essential fatty acids Optimal medium for delivery of fat soluble vitamins Good energy source Disadvantages: Increased incidence of chronic lung disease Hyperbilirubinemia Susceptibility to infection Protein: Helps lay down lean body mass Disadvantages:Cause nitrogen retention Electrolytes/Vitamins/Trace Elements
Monitoring of tolerance/efficacy • Carbohydrate: Monitor glucose levels Upper limit of 11mmol/l is acceptable • Lipids: Monitor triglyceride levels Upper limit of 2.0mmol/l is acceptable • Protein: Monitor urea levels Range 2-8mmol/l indicates protein requirements are met • Electrolytes: Serum Na (136-149mmol/l) is a marker of total sodium depletion which may slow growth Calcium & Magnesium should be monitored 2-3 times a week
INDICATIONS FOR TPN COMMENCEMENT • 9 babies were commenced on TPN. Indications:- <30/40 weeks gestation = 1 On ventilation >48 hrs = 1 Absent/reversed end diastolic flow = 1 <1500gms + absent/reversed end diastolic flow on doppler = 1 <30/40 weeks gestation + ventilated >48 hrs = 1 <30/40 weeks gestation, <1500gms + ventilated >48hrs = 1 Babies with none of the above indications but commenced on TPN = 3 2 babies had indications but did not receive TPN
INDICATOR 3 : TPN should continue until baby established on oral feeds n= 9 INDICATOR 2 : n = 9 • TPN is given within 2 days of decision to commence neonate on TPN All patients met this indicator
Indicator 4 n = 9 Carbohydrate and Protein should be increased as indicated on guidelines for parenteral nutrition All patients met this indicator • Indicator 5 n = 9 Lipids must always be included as an energy source within 48 hours of commencement of TPN All patients met this indicator
Indicator 6 n = 3 If baby has a) acute phase sepsis b) acidosis c) High unconjugated bilirubin > 200mmol/l lipid infusion should be reduced to 2g/kg/24hrs 1 patient with acute phase sepsis & acidosis had the lipid infusion reduced
Indicator 7 All neonates during first week of life should have a sodium range level within 136-149 mmol whilst on TPNException - Patient discharged/died within first week of life
Indicator 8 n = 9Baby will not have any complications whilst on TPN 1 baby had persistent metabolic acidosis 11% 89% No. of patients
Indicator 9 n = 9 Every neonate on TPN must have a TPN request form completed daily All patients met this indicator • Indicator 10 n = 9 For every TPN ordered a record sheet from pharmacy is received All patients met this indicator
Indicator 11 The amount of TPN prescribed should be documented on the patient’s drug chart n = 9 n = 9 Indicator 12 The amount of lipid prescribed should be documented on the patient’s drug chart
Indicator 13 n = 9 The amount of TPN should be documented in the nursing kardex All patients met this indicator • Indicator 14 n = 9 The amount of lipid given should be documented in the nursing kardex All patients met this indicator
Indicator 15 The amount of TPN prescribed and the actual amount given are the same n = 9 n = 9 Indicator 16 The amount of lipid prescribed and the actual amount given are the same
RECOMMENDATIONS • Make changes to indicator 1: Weight <1500gm + gestation <32/40 • Indicator 3 to be rephrased • Indicator 7 should read: all neonates during 1st week of life whilst on TPN should from the 2nd day of TPN have a sodium range of 136-149 • Combined doctor - nurse chart for TPN • Indicator 15 & 16 should be rephrased to include ‘……provided enteral feeds are not started’ • Add new indicators 1. TPN should have been given via a central line 2. All neonates on TPN should have BM < 11mmol/l Urea between 2-8mmol/l Triglycerides < 2.0mmol/l