Download
1 / 15
150 likes | 221 Views
This study explores delays in ART initiation, high loss to follow-up rates, and mortality among HIV-infected patients in Uganda. Findings highlight challenges and potential barriers in timely treatment initiation for ART-eligible patients. The research aims to address gaps in understanding outcomes of HIV care, including mortality, ART initiation, and disengagement from care. Implications suggest evaluating counseling requirements and treatment supporters to improve access to life-saving ART. Insights from this study have broader implications for HIV/AIDS care programs worldwide.

E N D
Failure to Initiate ART, Loss to Follow-up and Mortality among HIV-infected Patients during the pre-ART period in Uganda Elvin H. Geng1, Winnie Muyindike2, David V. Glidden1, Mwebesa B. Bwana2, Constantin T. Yiannoutsos3, Paula Braitstein3, Nicholas Musinguzi2, David R. Bangsberg4, Jeffrey N. Martin1 University of California San Francisco1; Mbarara University of Science and Technology, Mbarara, Uganda2; Indiana University3 and Harvard Medical School4 for the East Africa International Epidemiologic Databases to Evaluate AIDS
Engagement in care among ART Eligible Patients • For HIV-infected, ART eligible patients with CD4 counts < 250 cells/mm3, timely initiation is crucial and life saving. • To date, however, delays or failures in ART initiation are not well understood because loss to follow-up is high • Losses mean that the experience of ART-eligible patients – including the occurrence of mortality, ART initiation and disengagement from care – are partially observed. • We used a sampling based approach to assess outcomes in a setting where loss to follow-up is common: finding outcomes in a small but random sample of patients LTFU can “fill in the blanks.”
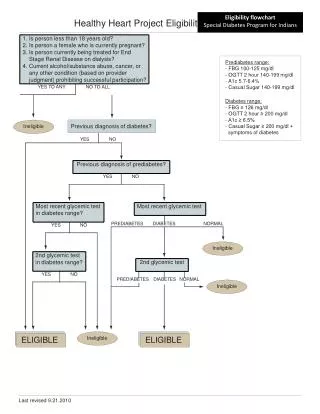
Objectives • We applied this sampling based approach at a prototypical scale-up ART clinic in Uganda: • High volume (200 patients/day) • Semi-rural environment • Implementing a simplified and standardized “public health approach” • CD4 testing is routinely available, viral load is not. • 2-3 counseling sessions and a treatment supporter are customary requirements for ART initiation.
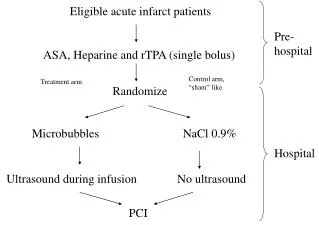
Methods • Patients • Adult, enrolled between Oct. 1, 2007 and Jan. 27, 2011 with a CD4-based indication for ART (i.e., CD4 < 250 cells/cc3) at the Immune Suppression Syndrome (ISS) Clinic in Mbarara, Uganda. • A random sample of patients in the community to ascertain updated vital status, whether they continued to see an HIV provider and whether they started ART at another clinic to better understand true outcomes. • Measurements • Patient data derived from data collected in the course of routine care • Analyses • Incidence of loss to follow-up (defined as 60 days late for an appointment) • Competing risks analysis of ART initiation (at original and other clinic), waiting for ART in care, disengagement from care (defined as 90 days without a visit to any facility) and mortality. • Sampled outcomes incorporated by a probability weight.
All ART- eligible Patients in Clinic Eligible patients with vital status ascertained by tracking (D) Patients lost to follow-up before ART (B) Patients sought by tracking (C) Patients who Continue in Care LTFU patients (B) Pw = Patients with ascertained outcomes (D)
Incidence of Loss to Follow-up before ART Initiation At 1-year: 21.0% (95% CI: 19.3%-22.6%).
2639 ART-eligible patients between 1-Oct-07 and 27-Jan-11 492 (19%) became lost to follow-up 163 (33%) Tracked 84 (52%) Alive 50 (31%) Died (18%) Not found 49 (58%) as reported by a proxy (i.e., family member) 35 (42%) as reported by patient him/herself 6 (17%) started ART at another clinic 16 (46%) seen a HIV provider at another clinic but not on ART 13 (37%) disengaged from care (i.e., not seen an HIV provider)
2639 ART-eligible patients between 1-Oct-07 and 27-Jan-11 492 (19%) became lost to follow-up 163 (33%) Tracked 84 (52%) Alive 50 (31%) Died (18%) Not found 49 (58%) as reported by a proxy (i.e., family member) 35 (42%) as reported by patient him/herself 6 (17%) started ART at another clinic 16 (46%) seen a HIV provider at another clinic but not on ART 13 (37%) disengaged from care (i.e., not seen an HIV provider)
Mortality in Random Sample of Patients Lost to Follow-up, N=134 At 1-year: 30.8% (95% CI: 22.9%-40.6%)
Sampling-based Estimate of Outcomes in all ART Eligible Patients Proportion Days since ART eligibility
Conclusions • Although ART initiation is rapid for a subgroup of “on-track” patients during the first 90 days after eligibility, a substantial fraction of ART eligible patients fail to initiate ART. • Loss to follow-up while waiting for ART is common at a prototypical ART clinic and mortality is high among those who fail to return to their originating clinic. • A substantial proportion of patients who fail to start ART continue to visit a clinic. • Year of ART eligibility, potentially reflecting drug supply, was found to influence ART initiation rates.
Implications • The final step from staging to ART in HIV/AIDS care and treatment programs may be accompanied by significant barriers and obstacles. • Standard procedures such as counseling requirements and treatment supporters, although widespread, should be evaluated to determine their risks vs. benefits. • If these observations are true elsewhere, in the roll out of ART to date, potentially over a million ART eligible patients failed to initiate ART in Africa, Asia, else where! • Strategies to fully engage ART-eligible patients represent a public health priority.
UCSF Jeffrey N. Martin Dave Glidden NIH Melanie Bacon Carolyn Williams Rosemary McKaig Indiana University Constantin Yiannoutsos Kara Wools Kaloustian Paula Braitstein Mbarara University Hassan Baryahikwa Mwebesa Bwana Nicholas Musinguzi Winnie Muyindike Harvard University David R. Bangsberg Acknowledgements