Download

1 / 47
880 likes | 2.02k Views
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master’s P rogrammes at the University of Pécs and at the University of Debrecen Identification number : TÁMOP-4.1.2-08/1/A-2009-0011.

E N D
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat theUniversity of Pécs and at the University of Debrecen Identificationnumber: TÁMOP-4.1.2-08/1/A-2009-0011
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat theUniversity of Pécs and at the University of Debrecen Identification number: TÁMOP-4.1.2-08/1/A-2009-0011 Dr. Judit Pongrácz Threedimensionaltissuecultures and tissueengineering – Lecture 9 Scaffoldfabrication
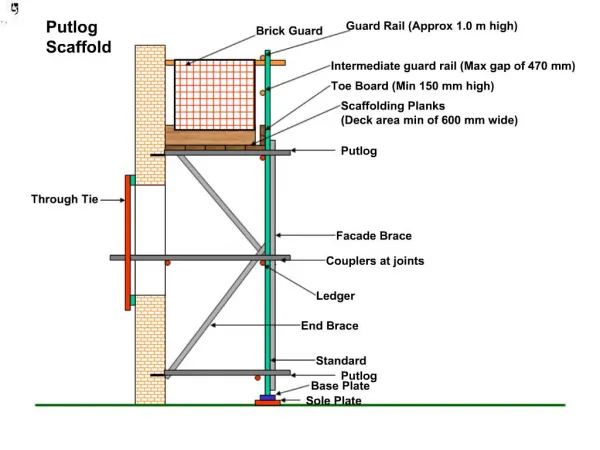
Basic criteria for scaffolds I Biocompatibility – to avoid immune reactions Surface chemistry – to support cellular functions Interconnected pores – cell infiltration and vascularization support Controlled biodegradability – to aid new tissue formation
Basic criteria for scaffoldsII Mechanical properties – structure and function maintenance after the implant and during remodeling Drug delivery – suitable for controlled delivery of drugs or bioactive molecules ECM interaction – supporting the formation of ECM after implantation ECM mimicking – ECM replacing role after implantation
Importance of scaffoldcharacteristics Scaffolds provide the 3D environment for cells Scaffolds temporarily replace the ECM after implantation Scaffolds are important in directing cellular differentiation Scaffold structure determines cell nutrition and mass transport into TE tissues
Solvent casting and particulate leaching (SCPL)I • Pour the dissolved scaffold into a mold filled with porogen • Evaporation of solvent in order to form scaffolds • Dissolving pore-forming particles from scaffolds • Scaffold layers: dip the mold into the dissolved scaffold material • Simple, easy and inexpensive technique • No special equipment is needed • Organic solvents are often toxic, difficult to eliminate contaminations
Solvent casting and particulate leaching (SCPL)II Solvent Mold Porogen Polymer Evaporation of solvent Porous structure is obtained Porogen is dissolved
Phase separation methods • Polymer is dissolved into the mixture of 2 non-mixing solvents • Saturated solutions at a higher temperature • Polymer-lean and polymer-rich phase separates • Lowering the temperature, the liquid-liquid phase is separated and the dissolved polymer is precipitating • The solvent is removed (extraction, evaporation, sublimation)
Advanced techniquesGas foaming • Specialized equipment needed • Pressure chamber filled with scaffold material • Scaffold is „dissolved” in supercritical CO2 • By lowering the pressure, physical condition turns to gas • Phase separation of dissolved scaffold occurs 10,000 solid supercritical fluid 1,000 liquid Pressure P (bar) 100 criticalpoint 10 gas triplepoint 1 200 250 300 350 400 Temperature T (K)
ElectrospinningI Syringe Polymer orcomposite solution Metallic needle High-voltage power supply Electrified jet V Collector
Electrospinning II • Specialized equipment required • Technique is very versatile • No extreme conditions (heat, coagulation, etc.) required • Many types of polymers are applicable, e.g. PLA, PLGA, silk fibroin, chitosan, collagen, etc. • Thickness, aspect ratio, porosity, fiber orientation are easily regulated
Advanced techniquesFibermesh Specialized equipment is needed Scaffold consists of (inter)woven fibres 2D or 3D scaffold structure are both available Pore size can be easily manipulated Versatile technique, scaffold material is broadly applicable and combinations can also be applied
Advanced techniquesSelf assembly Self assemblyis the spontaneous organization of molecules into a defined structure with a defined function Amphiphilic peptides in solutions form non-covalent bonds
Design of peptide ampholites Phosphoserine group to enhance mineralization (bone) RGD groups to provide integrin binding sites Cysteines to form intermolecular bridges GGG linker between the head and tail groups to increase flexibility
Advanced techniquesRapid prototyping Rapid prototyping is the automatic construction of physical objects using additive manufacturing technology. This technique allows fast scaffold fabrication with consistent quality, texture and structure. Expensive and specialized computer-controlled machinery needed.
Advanced techniquesFused deposition modeling (FDM) • Robotically guided extrusion machine • Extrudes plastic filament or other materials through a nozzle • Layers where the object should be solid and • Cross-hatching (using a different substance) for areas that will be removed later.
Advanced techniques Selective laser sintering (SLS) • Scaffold material in powder form, slightly below melting temperature • A computer-guided laser beam provides heat for the powder particles to sinter (weld without melting) • More new powder layers will be sintered as the piston moves downward and • The 3D structure of the object will be formed layer-by-layer
Selectivelasersintering(SLS) 1 2 3 Powder deliverysystem Scanner Laser Fabrication powderbed Object being fabricated Roller Build cylinder 4 5 7 Fabrication piston Powder deliverypiston Powder deliverypiston 6
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat theUniversity of Pécs and at the University of Debrecen Identification number: TÁMOP-4.1.2-08/1/A-2009-0011 Dr. Judit Pongrácz Threedimensionaltissuecultures and tissueengineering – Lecture 10 Biocompatibility
Biocompatibility - Definition • The ability of a material to perform with an appropriate host response in a specific application. • The biocompatibility of a scaffold or matrix for tissue-engineering products refers to the ability to perform as a substrate that will support the appropriate cellular activity, including the facilitation of molecular and mechanical signaling systems, in order to optimize tissue regeneration, without eliciting any undesirable effects in those cells, or inducing any undesirable local or systemic responses in the eventual host.
Biocompatibility -Recent views • Old concept: use of inert biomaterials that do not interact with the host tissues • New aims in biomaterial design: • Biomaterials actively interacting with host tissues • Biomaterials provoking positive physiological responses • Biomaterials supporting cell growth and differentiation
Biocompatibility of biomaterials • Natural derived materials are inherently biocompatible (e.g. collagen, fibrin, hyaluronic acid) • Xenogenic biomaterials have to be modified to achieve biocompatibility (e.g. bovine collagen has to be slightly digested before human application to remove the immunogenic sequences) • Nowadays recombinant human collagen is available • Other xenogenic materials (e.g. plant-derived polysaccharides have to be tested for biocompatibility • Synthetic materials have to be tested for biocompatibility
Biocompatibility -Terminology • Biodegradable: in vivo macromolecular degradation; no elimination of degradation products from the body • Bioabsorbable: macromolecular components enter in the body without metabolic change • Bioresorbable: macromolecular components are degraded and metabolized, reduction in molecular mass and excretion of the final product
Biocompatibility testing • Blood/material or tissue/material interface must be minimal. • Resistance to biodegeneration must be high. • The biomaterial must interact as a natural material would in the presence of blood and tissue. • Implantable materials should not: • Cause thrombus-formations • Destroy or sensitize the cellular elements of blood • Alter plasma proteins (including enzymes) so as to trigger undesirable reactions • Cause adverse immune responses • Cause cancer • Cause teratological effects • Produce toxic and allergic responses • Deplete electrolytes • Be affected by sterilization
Complications from incompatibility • Immune reaction towards the implanted material • Chronic inflammation • Scar tissue formation • Increased blood clotting (vascular graft incompatibility) • Graft insufficiency • Rejection
Normal woundhealing Woundhealingmay be divided into phases characterized byboth cellular population and cellular function: • Bloodclotting • Inflammation • Cellular invasion and remodeling
Foreign Body ReactionI The presence of the implant changes the healing response, and this is called the Foreign Body Reaction (FBR)consisting of: • Protein adsorption • Macrophages • Multinucleated foreign body giant cells • Fibroblasts • Angiogenesis Continuing presence of an implant may result in the attainment ofa final steady-state condition called resolution. There are 3 possible outcomes for the implant: • Resorption • Integration • Encapsulation (fibrosis)
Foreign Body ReactionII Bloodvessel Adsorbed plasma proteins mediate granulocyte and macrophage response Frustrated phagocytosis results in macrophage activation and giant cell formation Endothelium Monocyte Cell-migration Foreign body giantcell Macrophages Layercontaining fibroblasts and collagen Layer containing macrophages Biomaterial Biomaterial
Biomaterials • Temporary implants: • Temporary support of tissue regeneration and repair • Bone grafts, bioabsorbable surgical sutures • Permanent implants: • Long term physical integrity and mechanical performance • Long term replacement of organ function (heart valves, joints, etc.)
Bioinert materials • Poly-tetrafluor-ethylen (PTFE, Teflon®) • Inert in the body • Extremely low friction coefficient (0.05-0.10 vs. polished steel) • Biologically inert, no interaction with living tissue • Surface coating of joint prostheses and artificial heart valves
Silicone derivates • Silicones are polymers that contain Si besides of common C, H, N, O elements of biocompatible polymers. • Medical grade silicones: non-implantable, short- and long-term implantable • Silicone is used for catheters, tubing, breast implants, condoms
Biocompatible metals • Titanium alloys for joint replacement and dental implants • Excellent mechanical properties • Non-toxic and non-rejected • Uniquely capable of osseointegration • Hydroxyapatite coating before implantation enhances osseointegration
Hydroxyiapatite ceramics • Hydroxyapatite (HA) is naturally occurring in the bones and teeth • HA crystals are often combined with other polymers to form scaffolds • Microcrystalline HA is sold as a nutrition supplement to prevent bone loss • It is superior to CaCO3 in preventing osteoporosis
Poly-a-hydroxy-acids: bioabsorbable polymers • Most frequently used biomaterials • Main uses are resorbable sutures, drug delivery scaffolds and orthopedic fixtures • Polyester chains • Degradation by simple hydrolysis • The resulting a-hydroxy-acids are eliminated via metabolic pathways (e.g. citric acid cycle) or excreted unchanged with the urine
Degradation of poly-a-hydroxy-acids • Most frequently used poly-a-hydroxy-acids: • Poly-lactic acid (PLA) • Poly-glycolic acid (PGA) • Poly-capronolactone (PCL) • Degradation products enter into the citricacidcycle. H2O + (CH2)nCO(CH2)n C HO(CH2)n CO (CH2)COH O O O O Polyester Hydroxi-terminal Carboxy-terminal
Biodegradation of poly-a-hydroxy-acids H2O Esterase b-Hydroxybutyric acid PHB Serine Glycine Glycolic acid PGA H2O PDS Pyruvicacid Lacticacid PLA CO2 H2O Acetoacetate Acetyl-CoA PGA = poly(glycolicacid) PLA = poly(lacticacid) PDS = poly-(d-dioxane) PHB = poly(hydoroxybutyrate) Urine Citrate Citricacid cycle CO2 H2O Oxidativephosphorylation ATP
Poly-(Glycolic Acid), (PGA) • PGA is a rigid, highly crystalline material • Only soluble in highly apolar organic solvents • Main use as resorbable sutures (Dexon®) • SCPL method for scaffold fabrication • Bulk degradation • Natural degradation product (glycolic acid)
Poly-(Lactic Acid), PLA and PGA co-polymers • D, L isoform and racemic mixture • Most often the L isoform is used together with PGA→ PLGA copolymer • PLGA is one of the few polymers approved for human use • Copolymer mixtures of PGA and PLLA have various features thus allowing versatile application range in tissue engineering • Degradation rate and type depends on the composition of the co-polymers
Biodegradation of polylactides • Generally involves random hydrolysis of ester bonds • Type and duration of degradation depends on composition • Products are non-toxic, non-inflammatory • In case of larger orthopedic implants acidic degradation may produce toxic metabolites • Small particles may break off the implant inducing inflammation
Poly-(caprono-lactone), (PCL) • Semicrystalline polymer • Very slow degradation rate (pure PCL degrades in 3 years, copolymers withother caprones can be degraded more readily) • Used for drug delivery for longer periods • PCL is considered non-toxic and biocompatible material
Polymererosion • Water penetrates the bulk of the device, attacking the chemical bonds in the amorphous phase and converting long polymer chains into shorter water-soluble fragments. • This causes a reduction in molecular weight without the loss of physical properties as the polymer is still held together by the crystalline regions. Water penetrates the device leading to metabolization of the fragments and bulk erosion. • Surfaceerosion of the polymer occurs when the rate at which the water penetrating the device is slower than the rate of conversion of the polymer into water soluble materials.
Types of degradationinbiomaterials Surfaceerosion Bulkerosion Degradation Time
DegradationI • Biodegradable hydrogels: cleavage of chemical cross-links between water soluble polymer chains • Surface erosion is typical • Mass loss upon degradation is linear
DegradationII CH3 CH3 CH3 • Cleavage of the polymer backbone leading to water soluble monomers O O O O O O H2O −HO − CH − C − OH +OH − CH2 − C − OH −(CH − C − O − CH − C − O −)x−(CH2− C − O − CH2 − C − O)y− Krebbs cycle CO2 + H2O
DegradationIII • Polymer hydrophobicity: stability increases with increased hydrophobicity • Bulky substitutes (e.g. methyl group in PLA) increase degradation time (PGA<PLA) • Glass transition: Rubbery polymers above Tg have more chain mobility thus easier access for water • Crystallinity decreases, amorphous structure increases degradation time