Download
1 / 18
220 likes | 1.2k Views
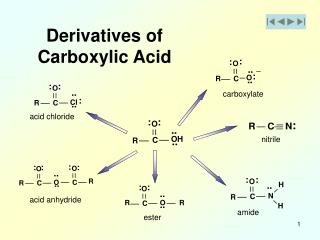
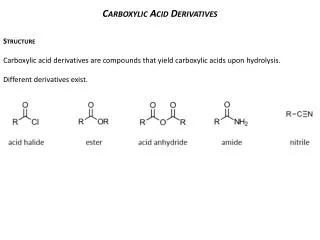
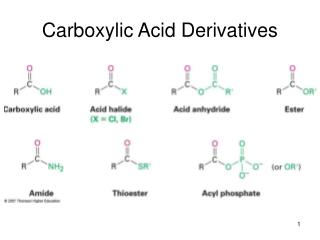
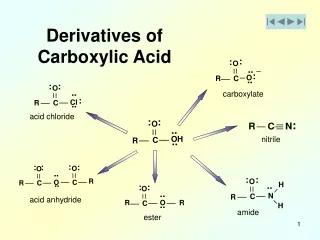
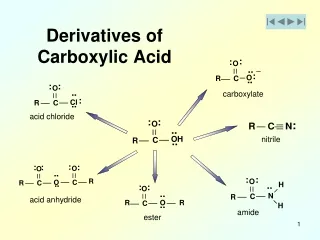
Propionic acid derivatives. Ibuprofen, naproxen, fenoprofen , flurbiprofen , oxaprozin ,→ anti-inflammatory, analgesic, and antipyretic.

E N D
Propionic acid derivatives Ibuprofen, naproxen, fenoprofen, flurbiprofen, oxaprozin,→ anti-inflammatory, analgesic, and antipyretic. These drugs are reversible inhibitors of the cyclooxygenasesbut Aspirin is a weak organic acid that is unique among the NSAIDs in that it irreversibly acetylates (and, thus, inactivates) cyclooxygenase, orally absorbed,bound to albumin chronic treatment of RA and osteoarthritis, GIT less effects than those of aspirin-dyspepsia,tinnitus,dizziness.
Acetic acid derivatives • Indomethacin, sulindac, etodolac • anti-inflammatory, analgesic, and antipyretic • reversibly inhibiting cyclooxygenase • acute gouty arthritis, ankylosingspondylitis, and osteoarthritis of the hip
Oxicam derivatives • Piroxicam, meloxicam , • Meloxicam inhibits both COX-1 and COX-2, and at low to moderate doses shows less GI irritation than piroxicam • They have long half-lives, which permit once-daily administration, and the parent drug as well as its metabolites are renally excreted in the urine. GI disturbances
Fenamates • Mefenamic acid, meclofenamate • have no advantages over other NSAIDs as anti-inflammatory agents. Their side effects, such as diarrhea, can be severe, and they are associated with inflammation of the bowel. Cases of hemolytic anemia
Heteroaryl acetic acids • Diclofenac→use in the treatment of RA, osteoarthritis, and ankylosingspondylitis. Diclofenac is more potent than indomethacin or naproxen. An ophthalmic preparation is also available. Diclofenac accumulates in synovial fluid, and the primary route of excretion for the drug and its metabolites is the kidney
Tolmetin→anti-inflammatory, antipyretic, and analgesic, half-life of 5 hours. It is 99 percent bound to plasma proteins, and metabolites can be found in the urine. Toxicities of these two agents are similar to those of the other NSAIDs
Ketorolac→is a potent analgesic but has moderate anti-inflammatory effects. It is available for oral administration, for intramuscular use in the treatment of postoperative pain, and for topical use for allergic conjunctivitis. Ketorolac undergoes hepatic metabolism, and the drug and its metabolites are eliminated via the urine. Ketorolac is indicated for short-term relief of moderate to severe pain for up to 5 days after the first dose is administered via IV or intramuscular dosing
Nabumetone • treatment of RA and osteoarthritis and is associated with a low incidence of adverse effects. Nabumetone is hepatically metabolized by the liver to the active metabolite, which displays the anti-inflammatory, antipyretic, and analgesic activity. The active metabolite is then hepatically metabolized to inactive metabolites with subsequent renal elimination.
Celecoxib • Celecoxib is approved for treatment of RA, osteoarthritis, and pain. Unlike aspirin, celecoxib does not inhibit platelet aggregation and does not increase bleeding time. Celecoxib has similar efficacy to NSAIDs in the treatment of pain and the risk for cardiovascular events. Celecoxib, when used without concomitant aspirin therapy, has been shown to be associated with less GI bleeding and dyspepsia;
Pharmacokinetics→Celecoxib orally absorbed, reaching a peak concentration in about 3 hours. It is metabolized in the liver by cytochrome P450 and is excreted in the feces and urine. Its half-life is about 11 hours; thus, the drug is usually taken once a day, celecoxib should be avoided in patients with severe hepatic and renal disease.
Adverse effects • dyspepsia, diarrhea, and abdominal pain are the most common adverse effects. Celecoxib should be avoided in patients with chronic renal insufficiency, severe heart disease, volume depletion, and/or hepatic failure
Acetaminophen • inhibits prostaglandin synthesis in the CNS,its antipyretic and analgesic properties. Acetaminophen has less effect on cyclooxygenase in peripheral tissues, which accounts for its weak anti-inflammatory activity. Acetaminophen does not affect platelet function or increase blood clotting time.
Therapeutic uses • analgesic and antipyretic effects of aspirin for those patients with gastric complaints, those in whom prolongation of bleeding time would be a disadvantage, or those who do not require the anti-inflammatory action of aspirin
Acetaminophen is the analgesic/antipyretic of choice for children with viral infections or chickenpox (recall that aspirin increases the risk of Reye's syndrome). Acetaminophen does not antagonize the uricosuric agents probenecid or sulfinpyrazone and, therefore, may be used in patients with gout who are taking these drugs.
Pharmacokinetics • Acetaminophen is rapidly absorbed from the GI tract. A significant first-pass metabolism occurs in the luminal cells of the intestine and in the hepatocytes. Under normal circumstances, acetaminophen is conjugated in the liver to form inactive glucuronidated or sulfated metabolites
A portion of acetaminophen is hydroxylated to form N-acetylbenzoiminoquinone a highly reactive and potentially dangerous metabolite that reacts with sulfhydryl groups. At normal doses of acetaminophen, the N-acetylbenzoiminoquinone reacts with the sulfhydryl group of glutathione, forming a nontoxic substance and its metabolites excretes in urine.
Adverse effects • Skin rash, alterations in the leukocyte count, Renal tubular necrosis and hypoglycemic coma are rare complications of prolonged, large-dose therapy. • acetaminophen, the available glutathione in the liver becomes depleted, and N-acetylbenzoiminoquinone reacts with the sulfhydryl groups of hepatic proteins, forming covalent bonds
Hepatic necrosis, very serious and potentially life-threatening condition, can result. Renal tubular necrosis may also occur. [Note: Administration of N-acetylcysteine, which contains sulfhydryl groups to which the toxic metabolite can bind, can be lifesaving if administered within 10 hours of the overdose,in liver disease it is contra-indicated.