Download
1 / 1
10 likes | 119 Views
Mediators of Combined Cardiorespiratory Biofeedback and Dialectical Behavioral Skills Therapy for Treating Major Depressive Disorder and Low Heart Rate Variability Following Myocardial Infarction. Milton Brown, Priya Chaudhri, and Richard Gevirtz

E N D
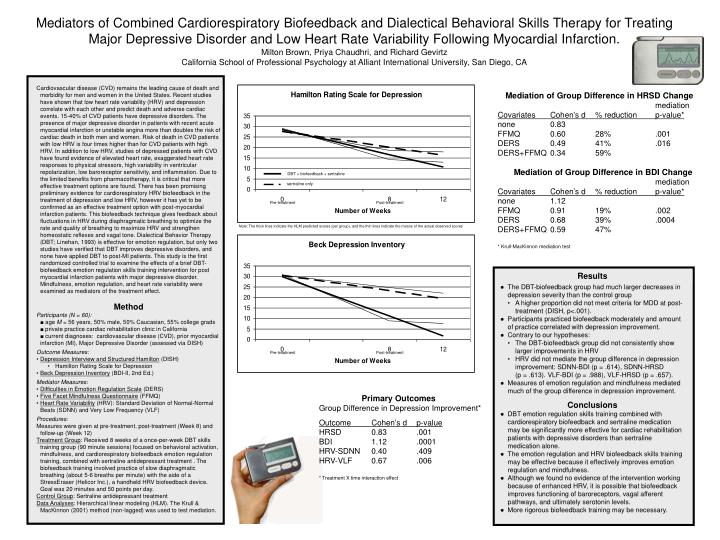
Mediators of Combined Cardiorespiratory Biofeedback and Dialectical Behavioral Skills Therapy for Treating Major Depressive Disorder and Low Heart Rate Variability Following Myocardial Infarction. Milton Brown, Priya Chaudhri, and Richard Gevirtz California School of Professional Psychology at Alliant International University, San Diego, CA • Cardiovascular disease (CVD) remains the leading cause of death and morbidity for men and women in the United States. Recent studies have shown that low heart rate variability (HRV) and depression correlate with each other and predict death and adverse cardiac events. 15-40% of CVD patients have depressive disorders. The presence of major depressive disorder in patients with recent acute myocardial infarction or unstable angina more than doubles the risk of cardiac death in both men and women. Risk of death in CVD patients with low HRV is four times higher than for CVD patients with high HRV. In addition to low HRV, studies of depressed patients with CVD have found evidence of elevated heart rate, exaggerated heart rate responses to physical stressors, high variability in ventricular repolarization, low baroreceptor sensitivity, and inflammation. Due to the limited benefits from pharmacotherapy, it is critical that more effective treatment options are found. There has been promising preliminary evidence for cardiorespiratory HRV biofeedback in the treatment of depression and low HRV, however it has yet to be confirmed as an effective treatment option with post-myocardial infarction patients. This biofeedback technique gives feedback about fluctuations in HRV during diaphragmatic breathing to optimize the rate and quality of breathing to maximize HRV and strengthen homeostatic reflexes and vagal tone. Dialectical Behavior Therapy (DBT; Linehan, 1993) is effective for emotion regulation, but only two studies have verified that DBT improves depressive disorders, and none have applied DBT to post-MI patients. This study is the first randomized controlled trial to examine the effects of a brief DBT-biofeedback emotion regulation skills training intervention for post myocardial infarction patients with major depressive disorder. Mindfulness, emotion regulation, and heart rate variability were examined as mediators of the treatment effect. • Method • Participants (N = 60): • ■ age M = 56 years, 50% male, 50% Caucasian, 55% college grads • ■ private practice cardiac rehabilitation clinic in California • ■ current diagnoses: cardiovascular disease (CVD), prior myocardial infarction (MI), Major Depressive Disorder (assessed via DISH) • Outcome Measures: • Depression Interview and Structured Hamilton (DISH) • Hamilton Rating Scale for Depression • Beck Depression Inventory (BDI-II, 2nd Ed.) • Mediator Measures: • Difficulties in Emotion Regulation Scale (DERS) • Five Facet Mindfulness Questionnaire (FFMQ) • Heart Rate Variability (HRV): Standard Deviation of Normal-Normal Beats (SDNN) and Very Low Frequency (VLF) Procedures: Measures were given at pre-treatment, post-treatment (Week 8) and follow-up (Week 12) Treatment Group: Received 8 weeks of a once-per-week DBT skills training group (90 minute sessions) focused on behavioral activation, mindfulness, and cardiorespiratory biofeedback emotion regulation training, combined with sertraline antidepressant treatment . The biofeedback training involved practice of slow diaphragmatic breathing (about 5-6 breaths per minute) with the aide of a StressEraser (Helicor Inc.), a handheld HRV biofeedback device. Goal was 20 minutes and 50 points per day. Control Group: Sertraline antidepressant treatment Data Analyses: Hierarchical linear modeling (HLM). The Krull & MacKinnon (2001) method (non-lagged) was used to test mediation. • Mediation of Group Difference in HRSD Change • mediation • Covariates Cohen’s d % reduction p-value* • none 0.83 • FFMQ 0.60 28% .001 • DERS 0.49 41% .016 • DERS+FFMQ 0.34 59% • Mediation of Group Difference in BDI Change • mediation • Covariates Cohen’s d % reduction p-value* • none 1.12 • FFMQ 0.91 19% .002 • DERS 0.68 39% .0004 • DERS+FFMQ 0.59 47% • * Krull-MacKinnon mediation test DBT + biofeedback + sertraline sertraline only Pre-treatment Post-treatment Note: The thick lines indicate the HLM predicted scores (per group), and the thin lines indicate the means of the actual observed scores • Results • ● The DBT-biofeedback group had much larger decreases in depression severity than the control group • A higher proportion did not meet criteria for MDD at post-treatment (DISH, p<.001). • ● Participants practiced biofeedback moderately and amount of practice correlated with depression improvement. • ● Contrary to our hypotheses: • The DBT-biofeedback group did not consistently show larger improvements in HRV • HRV did not mediate the group difference in depression improvement: SDNN-BDI (p = .614), SDNN-HRSD (p = .613). VLF-BDI (p = .988), VLF-HRSD (p = .657). • ● Measures of emotion regulation and mindfulness mediated much of the group difference in depression improvement. • Conclusions • ● DBT emotion regulation skills training combined with cardiorespiratory biofeedback and sertraline medication may be significantly more effective for cardiac rehabilitation patients with depressive disorders than sertraline medication alone. • ● The emotion regulation and HRV biofeedback skills training may be effective because it effectively improves emotion regulation and mindfulness. • ● Although we found no evidence of the intervention working because of enhanced HRV, it is possible that biofeedback improves functioning of baroreceptors, vagal afferent pathways, and ultimately serotonin levels. • ● More rigorous biofeedback training may be necessary. Pre-treatment Post-treatment • Primary Outcomes • Group Difference in Depression Improvement* • Outcome Cohen’s d p-value • HRSD 0.83 .001 • BDI 1.12 .0001 • HRV-SDNN 0.40 .409 • HRV-VLF 0.67 .006 • * Treatment X time interaction effect






















