Download
1 / 30
430 likes | 1.27k Views
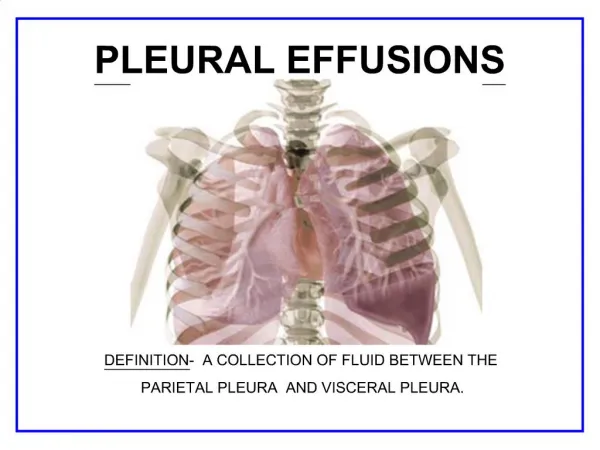
PLEURAL EFFUSIONS. http://intensivecare.hsnet.nsw.gov.au/five/images/pleural%20effusion%20CXR%202.jpg. DEFINITION - An abnormal accumulation of excess pleural fluid in the pleural cavity. ANATOMY AND PHYSIOLOGY IN A HEALTHY LUNG. The Right Lung -Makes up 56% of the total lung volume

E N D
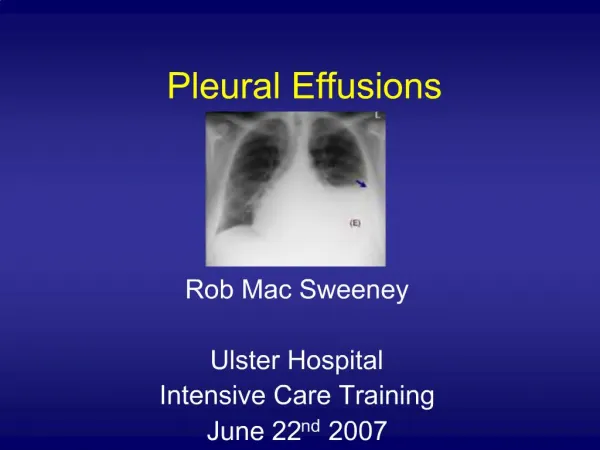
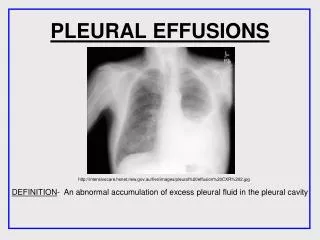
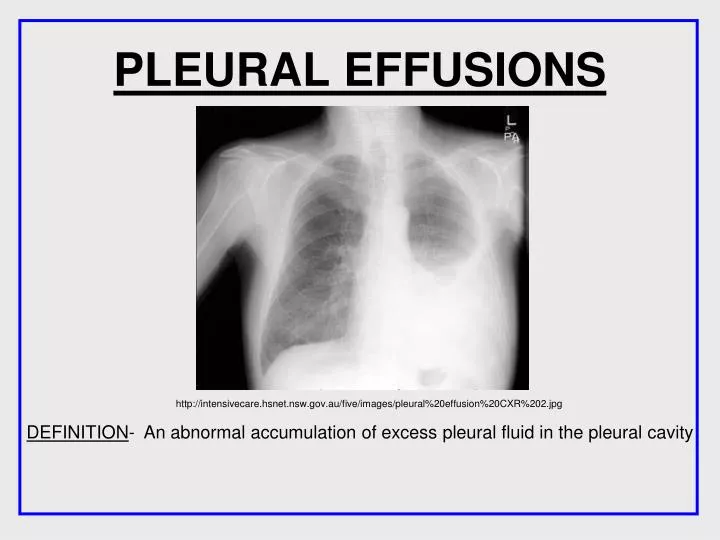
PLEURAL EFFUSIONS http://intensivecare.hsnet.nsw.gov.au/five/images/pleural%20effusion%20CXR%202.jpg DEFINITION- An abnormal accumulation of excess pleural fluid in the pleural cavity
ANATOMY AND PHYSIOLOGY IN A HEALTHY LUNG The Right Lung -Makes up 56% of the total lung volume -Three lobes-the superior, middle and inferior, which are separated by the horizontal fissure and the oblique fissure. Horizontal fissure The Left Lung -Makes up 44% of the total lung volume -Two lobes which are separated by the oblique fissure. Oblique fissure Oblique fissure http://fitsweb.uchc.edu/ctanatomy/chest/review/segments-posterior.html
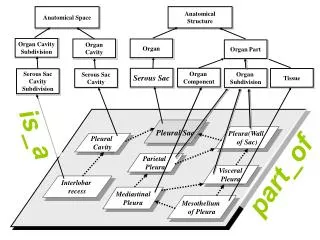
The main anatomy affected by pleural effusions are the layers in the Lung • There are two layers-the parietal pleura and the visceral pleura. • At the Hilum, the parietal pleura folds back on itself to become the visceral pleura. • The mesothelium is a membrane that forms the lining of the • pleura. • A simple squamous epithelium • The pleural fluid contains – • Glucose • Mesothelial cells • Macrophages • Lymphocytes • Sodium, potassium and calcium • Lactate Dehydrogenase http://www.nature.com/modpathol/journal/v18/n2/images/3800278f1.jpg
ANATOMY OF A HEALTHY LUNG ANATOMY OF A LUNG WITH A PLEURAL EFFUSION http://www.themesotheliomalibrary.com/pleural-effusions3.gif A pleural effusion is an accumulation of fluid between the parietal pleura and the visceral pleura.
ANATOMY OF A LUNG WITH A PLEURAL EFFUSION • The fluid accumulates due to the over production of pleural fluid by the mesothelial cells and separates the visceral and parietal pleura. • This fluid can not be drained by the lymphatic system, and so • therefore continues to accumulate, resulting in a pleural effusion. • The accumulation of fluid may also be due to changes in • hydrostatic pressure or oncotic pressure. • Other changes to anatomy include- • - Pleural thickening • - Mediastinal Pleural thickening • - Diaphragmatic Pleural thickening • - Presence of Pleural nodules • - Increase in pressure, due to the increase in fluid www.ncbi.nlm.nih.gov
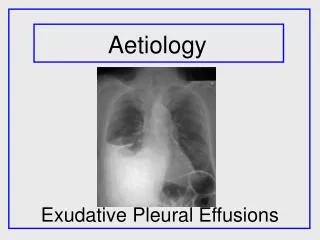
Aetiology http://www.eurorad.org/eurorad/view_figure.php?pubid=4921&figid=10954&nr=1
Oncotic – fluid pulled in Hydrostatic Pressure – fluid pushed out Increase peritoneal fluid
Transudates Main causes: Other possible causes: • Congestive heart failure • Cirrhosis • Nephrotic syndrome • Hypoalbuminemia • Myxedema- Severe hypothyroidism • Atelectasis - Collapse of lung
What is an Exudate? Transudative and exudative pleural effusions are distinguished by measuring the lactate dehydrogenase (LDH) and protein levels in the pleural fluid. LDH is an enzyme which is important to the production of energy in cells. When cells die LDH is released and escapes into the blood. High levels of LDH indicate infection or cancer are present A cloudy, viscous fluid containing proteins and cellular debris which has escaped from blood vessels and has been deposited in tissues, or on tissue surfaces, usually as a result of inflammation. • Fluid extracted from pleura via thorococentesis as show in the image on this slide. http://medical-dictionary.thefreedictionary.com/thoracentesis
Causes of Exudative Pleural Effusions Parapneumonic causes Malignancy (carcinoma, lymphoma, mesothelioma) Pulmonary embolism Collagen-vascular conditions (rheumatoid arthritis, lupus) Tuberculous Asbestos exposure Trauma (haemathorax) Postcardiac injury syndrome Esophageal perforation Radiation pleuritis Drug use Once an exudative pleural effusion has been established from the fluid test, the causes can be investigated. An exudative pleural effusion is not a pathology in itself and is always caused by something else such as:
Mesothelioma • The Most common cause of mesothelioma is inhalation of asbestos fibres. • Asbestos fibres are very fine and sharp and once they have been inhaled they cannot be exhaled or coughed out http://www.mesotheliomacenter.org/about/pleural-mesothelioma.php Once asbestos fibres become deposited in the pleura they irritate and inflame the mesothelial cells affecting the adherens junctions allowing exudative fluid to flow into the pleural space. http://www.asbestosclaimlawyermaryland.com/asbestosis-claim-asbestos-diseases
Diagnosis of Pleural Effusions Medical history Physical examination Plain film chest x-ray – first line imaging CT Ultrasound MRI Diagnosing Pleural Effusions through Imaging
Meniscus shaped upper border Clear right side hemi-diaphragm and sharp costophrenic angle Area of homogenous Whiteness First line imaging – Chest x-ray Features on a PA radiograph http://intensivecare.hsnet.nsw.gov.au/five/images/pleural%20effusion%20CXR%202.jpg
These are approximations Berman, L., De Lacey, G and Raby, N. (2008) Accident and Emergency Radiology a survival guide, 2nd edition. Saunders, Elsevier. P262-263
Entire white-out of right hemi-thorax The hearthas been pushed towardsthe left side A large right side pleural effusion
Lateral decubitus chest radiograph Free layering pleural effusion emedicine.medscape.com/article/299959-media
Pleural Effusion Diagnosis through CT Imaging medical.siemens.com
Heart Right Lung Left Lung Crescent-shaped pleural effusion Ribs Aorta
Loculated effusion (elliptical, pointed margins) in left major fissure
Irregular soft-tissue thickening Mass, right upper lobe Pleural effusion Aorta
Liver Ascites Spleen Diaphragm Pleuraleffusion Right Lung
Ultrasound Second point of imaging No radiation Small effusions missed on CXR Used to guide thoracocentisis Dark space on image http://www.cardiovascularultrasound.com/content/figures/1476-7120-6-16-7-l.jpg
Patient position http://img.youtube.com/vi/3zbKKedwZ94/0.jpg • Patient seated, arms folded, leaning forward • Unwell patient imaged semi-supine
MRI Not used to image pleural effusion Incidental finding
Treatment Needed if patient becomes breathless Small effusions are left and ‘observed’ Usually directed at underlying cause (antibiotics for pneumonia) Underlying cause treated effusion will go away for good If not it will return within few weeks
Thoracocentisis • Invasive procedure • Removes fluid from pleural space • Allows lung to expand, making breathing easier • Guided using ultrasound National Heart, Lung and Blood Institute
Pleurodesis • Chemical inserted into pleural space • Parietal and visceral layers become irritated • Closes space • Painful Pleuroperitoneal Shunt • Internal shunt • Fluid drains from chest into abdominal cavity Pleurectomy • Operation to remove the pleura • Most severe cases
Goldberg, Persky and White (2009) ‘Mesothelioma Centre’ [Online rescource] available at:http://www.mesotheliomacenter.org/about/pleural-mesothelioma.php accessed 28/12/2009 Daniel L. Miller (2009) ‘Extrapleural Pneumonectomy’ CTSnet [online rescourse] Available at: http://www.ctsnet.org/sections/clinicalresources/thoracic/expert_tech-7.html accessed 2812/2009 Jeffrey Rubins (2009) ‘pleural effusion’ eMedicine [online rescource] Available at: http://emedicine.medscape.com/article/299959-overview accessed: 28/12/2009 National Macmillan Mesothelioma Resource Centre (2008) ‘mesothelioma uk’ [online rescource] available at http://www.mesothelioma.uk.com/index.php?pageno=18 accessed 28/12/2009 Cancer research UK 2009 ‘mesothelioma’ [online rescource] available at http://www.cancerhelp.org.uk/type/mesothelioma/index.htm accessed:28/12/2009 Victor L Roggli, thomas A Sporn and tim d ovry (2004) ‘pathology of asbestos associated disease’2nd Edition, springer, New York. Harvey I Pass, Nicholas J Vogelzang Michele Carbone (2005) ‘Malignant mesothelioma- advances in pathogenesis, diagnosis and translational therapies’ Springer, New York Harvey Pass (2008) ‘All about malignant mesothelioma’[Online resource] available at http://www.allaboutmalignantmesothelioma.com/pleural-plaque.htm accessed 8/1/2010 Peter Armstrong and Martin Wastie (2004) ‘Diagnostic imaging’ 5th ed , Wiley Blackwell, Edinburgh REFERENCES
http://intensivecare.hsnet.nsw.gov.au/five/images/pleural%20effusion%20CXR%202.jpghttp://intensivecare.hsnet.nsw.gov.au/five/images/pleural%20effusion%20CXR%202.jpg