Download
1 / 17
240 likes | 540 Views
Treatment of hypertensive patients with heart failure. Jamil Mayet Department of Cardiology and The Peart-Rose Clinic St Mary’s Hospital, NHLI Imperial College, London, UK. Age-adjusted risk of congestive heart failure by hypertensive status. <140/90 >160/90. Kannel WB. Framingham.

E N D
Treatment of hypertensive patients with heart failure Jamil Mayet Department of Cardiology and The Peart-Rose Clinic St Mary’s Hospital, NHLI Imperial College, London, UK
Age-adjusted risk of congestive heart failure by hypertensive status <140/90 >160/90 Kannel WB. Framingham
The progression from hypertension to congestive heart failure • 5143 subjects in Framingham study • 392 new cases of clinical CCF after mean follow up of 20 years • In 91% hypertension antedated CCF • MI present in 52% of hypertensive men and 34% of hypertensive women with CCF • Median survival after CCF diagnosis in ht 1.37 years in men and 2.48 in women Levy et al. JAMA 1996;275:1557-62
Age-adjusted BP parameters and CHF risk Hazard Ratio 120-139 140-159 70-79 80-89 54-67 <120 >159 <70 >89 <54 >67 Chae et al. JAMA1999;281:634-9
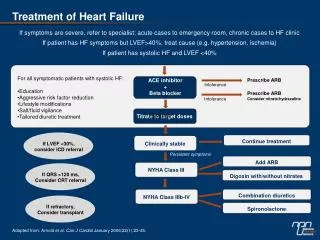
Treatments that improve CCF and lower BP • Non-pharmacological (salt restriction, exercise) • ACE inhibitors (SOLVD, CONSENSUS) • Beta blockers (CIBIS 2, MERIT-HF) • Diuretics
Age-adjusted BP parameters and CHF risk Hazard Ratio 120-139 140-159 70-79 80-89 54-67 <120 >159 <70 >89 <54 >67 Chae et al. JAMA199;281:634-9
Arterial stiffening in hypertension • Increased PW velocity with early wave reflection • Increased central systolic pressure and lower diastolic pressure • Discrepancy between central and peripheral pressures lessened • Therefore peripheral BP underestimates central effects
Reducing arterial stiffness as a therapeutic goal • Later wave reflection reduces peak central pressure which is caused by summation of systolic wave and reflected wave • In periphery peak pressure is not a summation wave and so there is less of a decrease • Reducing stiffness causes preferential decrease in central compared with peripheral pressures
Non-pharmacological approaches to reducing arterial stiffness • Increased arterial stiffness in obese subjects with improvement following weight reduction • Moderate aerobic exercise increases arterial compliance • Subjects with high salt intake have better arterial distensibility than those with low intake. • Improvement following salt restriction
Stiffness LV Outcome impact regression data ?+ + No a -blockers +++ +++ No ACE-inhibitors + + Yes b -blockers ++ ?? No b -blockers ‘extra’ +++ ++ Yes ++ Ca antagonists + +/++ Yes + thiazides Relation between vascular and LV impacts of antihypertensives
Diastolic heart failure • Symptoms/signs of heart failure with normal or mildly impaired LV systolic function • Prevalence depends on clinical definition of heart failure • May be up to 30% of cases with heart failure • Diastolic dysfunction in hypertensives is very common, particularly in those with LVH
Pathophysiology of diastolic dysfunction • Impaired relaxation • Energy dependent and sensitive to ischaemia • Coronary artery disease • Microvascular ischaemia (arteriolar rarefaction, arteriole wall thickening, perivascular fibrosis, endothelial dysfunction, relative myocyte hypertrophy) • Decreased compliance • Increase in myocardial collagen
Treatment of diastolic dysfunction • Treat underlying cause eg coronary intervention • Most patients are elderly and hypertensive +/- LVH • Beta blockers may improve filling by reducing heart rate and prolonging diastole; also may reduce myocardial O2 demand and regress LVH • Ca antagonists, particularly rate limiting, may have similar effects • BUT VERY LITTLE FUNCTIONAL DATA
Treatment of diastolic dysfunction • Beta blockers and Ca antagonists unlikely to be effective when restrictive physiology with raised LA pressure • Drugs that reduce fibrosis and reduce LA pressure likely to be effective • ACEI, AII antagonists, spironolactone, diuretics • BUT VERY LITTLE FUNCTIONAL DATA
Treatment of diastolic dysfunction • Echo guided strategy • Impaired relaxation • Verapamil • Beta-blockers • Restriction with increased LA pressure • ACEI • AII blockers • Diuretics (spironolactone)