Download
1 / 32
320 likes | 333 Views
Primary Prevention of Acute Coronary Events with Lovastatin in Men and Women with Average Cholesterol Levels Results of AFCAPS/TexCAPS.

E N D
Primary Prevention of Acute Coronary Events with Lovastatin in Men and Women with Average Cholesterol LevelsResults of AFCAPS/TexCAPS John R. Downs, Michael Clearfield, Stephen Weis, Edwin Whitney, Deborah R. Shapiro, Polly A. Beere, Alexandra Langendorfer, Evan A. Stein, William B. Kruyer, Antonio M. Gotto; for the AFCAPS/TexCAPS Research Group JAMA 1998;279:1615-1622
LDL-C Major Statin Trials 4S WOSCOPS CARE LIPID AFCAPS/ TexCAPS 1º Prevention 2º Prevention Gotto, et. al. AHA Nov ’97 Preliminary Results
Objective • To compare lovastatin with placebo for prevention of the first acute major coronary event: • unstable angina, fatal and non-fatal MI and sudden cardiac death in a cohort of men and women without clinically evident atherosclerotic CVD, who have average TC and LDL-C and below-average HDL-C. JAMA 1998;279:1615-1622
AFCAPS/TexCAPSStudy Design • Design: • Randomized, double-blind, placebo-controlled trial • Setting: • Outpatient clinics in Texas • Participants: • 5608 men and 997 women with at baseline, average TC (221 mg/dL) and LDL-C (150 mg/dL) and below-average HDL-C (37 mg/dL). • Intervention: • Lovastatin (20-40 mg daily - to achieve an LDL-C of < 110 mg/dL) or placebo in addition to a low-saturated fat, low-cholesterol diet. JAMA 1998;279:1615-1622
Primary Endpoint • First Acute Major Coronary Event defined as: • Unstable Angina Pectoris* • Fatal or Non-fatal MI • Sudden Cardiac Death *Unstable Angina Endpoint Criteria Clinical history with hospitalization, reversible ischemic ECG changes, + thallium ETT, cardiac catheterization: > 90% stenosis in major epicardial coronary artery. JAMA 1998;279:1615-1622
Secondary Endpoints • Fatal or Non-Fatal Coronary Revascularization • Fatal or Non-Fatal MI • Unstable Angina • Fatal or Non-Fatal Cardiovascular Events • Fatal or Non-Fatal Coronary Events • Cardiovascular Mortality • CHD Mortality JAMA 1998;279:1615-1622
Tertiary Endpoints • Total Mortality • Non-Cardiovascular Mortality • Fatal and Non-Fatal Cancer • Discontinuation of Medication because of Adverse Effects JAMA 1998;279:1615-1622
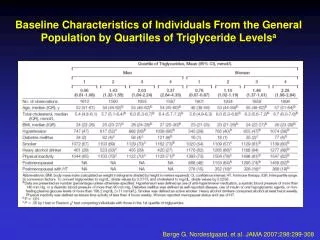
Baseline Demographics AFCAPS/TexCAPS NHANES III* Gender Women ( 997) 15% 42% Race White - 89% 85% Hispanic - 7% 7% Black - 3% 8% Mean Age 58 + 7 y.o. 60 + 8 y.o. Men (45-73) 57 + 7 y.o. 57 + 8 y.o. Women (55-73) 63 + 5 y.o. 64 + 5 y.o. > 65 at Randomization 21% 33% JAMA 1998;279:1615-1622
Risk Factors AFCAPS/TexCAPSNHANES III* Hypertension 22% 35% Active Smoker 13% 26% NIDDM 2% 4% Family History 15% 9% HDL-C < 35 mg/dl 35% 13% JAMA 1998;279:1615-1622
Baseline Lipid LevelsCompared with U.S. Reference Population Based Upon NHANES III JAMA 1998;279:1615-1622 1 Percentile ranks from US NHANES III reference population for study population averages 2 Men aged 45-73, and women aged 55-73, without cardiovascular disease
Year 1 Lipids Lovastatin 183.7 + 23.8 114.6 + 20.1 39.3 + 8.0 142.8 + 72.8 3.0 + 0.8 4.8 + 1.0 Placebo 228.1 + 27.7 156.4 + 24.5 37.5 + 7.9 162.8 + 82.1 4.3 + 1.1 6.3 + 2.5 Mean TC Mean LDL-C Mean HDL-C Median TG Ratios Mean LDL-C/HDL-C Mean TC/HDL-C JAMA 1998;279:1615-1622
Percent Change in Lipid Parameters Baseline to Year 1 p-value < 0.001 for all lovastatin treatment groups 42% of lovastatin patients achieved LDL-C goal of < 110 mg/dL (placebo 3%) 81% of lovastatin patients achieved LDL-C goal of < 130 mg/dL (placebo 12%) TC LDL HDL TG TC/HDL LDL/HDL JAMA 1998;279:1615-1622
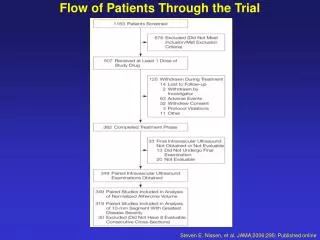
Primary Endpoint ~ First Acute Major Coronary Event* 0.06 *Includes unstable angina, fatal and non-fatal MI & sudden cardiac death 0.05 Placebo 37% Risk Reduction (p < 0.001) 0.04 Cumulative Incidence 0.03 Lovastatin 0.02 0.01 0.00 0 1 2 3 4 5 5+ Years Years of Follow-up # At Risk Lovastatin N=3304 N=3270 N=3228 N=3184 N=3134 N=1688 Placebo N=3301 N=3251 N=3211 N=3159 N=3092 N=1644 JAMA 1998;279:1615-1622
Primary EndpointRisk of First Acute Major Coronary Event by Year Fatal & Non-fatal MI, Unstable Angina, Sudden Cardiac Death reduced by 37% (p < 0.0008) Poster Presentation at the 1998 ACC Meeting, Atlanta GA
Lovastatin Reduced the Risk of First Acute Major Coronary Events > Median by Age N=3180 Men N=5608 Women N=997 Smokers N=818 Hypertension N=1448 Diabetes N=156 Poster Presentation at the 1998 ACC Meeting, Atlanta GA
Lovastatin Reduced the Risk of First Acute Major Coronary Events in All Baseline LDL Tertiles Baseline LDL Tertiles Poster Presentation at the 1998 ACC Meeting, Atlanta GA
AFCAPS/TexCAPSRole of Baseline LDL on Outcomes Baseline LDL Level (mg/dL) JAMA 1998;279:1615-1622
AFCAPS/TexCAPSRole of Baseline HDL on Outcomes JAMA 1998;279:1615-1622
AFCAPS/TexCAPSRole of Baseline HDL on Outcomes Baseline HDL Level (mg/dL) JAMA 1998;279:1615-1622
# At Risk # At Risk Lovastatin N=3304 N=3260 N=3206 N=3147 N=3088 N=1651 Lovastatin N=3304 N=3281 N=3249 N=3214 N=3174 N=1717 Placebo N=3301 N=3242 N=3187 N=3124 N=3045 N=1615 Placebo N=3301 N=3270 N=3237 N=3200 N=3148 N=1692 # At Risk # At Risk Lovastatin N=3304 N=3264 N=3215 N=3160 N=3106 N=1666 Lovastatin N=3304 N=3281 N=3250 N=3217 N=3174 N=1707 Placebo N=3301 N=3246 N=3201 N=3141 N=3069 N=1634 Placebo N=3301 N=3267 N=3240 N=3205 N=3150 N=1678 Secondary Endpoint Analyses Cardiovascular Events* Fatal and Non-Fatal MI 0.08 0.03 25% Risk Reduction (p = 0.003) Placebo 0.07 40% Risk Reduction (p = 0.002) Placebo 0.06 0.02 0.05 Cumulative Incidence Cumulative Incidence 0.04 Lovastatin Lovastatin 0.03 0.01 0.02 0.01 0.00 0.00 0 1 2 3 4 5 5+ years 0 1 2 3 4 5 5+ years Years of Follow-up Years of Follow-up Unstable Angina Coronary Events* 0.03 0.07 0.06 25% Risk Reduction (p = 0.006) Placebo Placebo 32% Risk Reduction (p = 0.02) 0.05 0.02 0.04 Cumulative Incidence Cumulative Incidence 0.03 Lovastatin 0.01 Lovastatin 0.02 0.01 0.00 0.00 0 1 2 3 4 5 5+ years 0 1 2 3 4 5 5+ years Years of Follow-up Years of Follow-up JAMA 1998;279:1615-1622
# At Risk Lovastatin N=3304 N=3277 N=3237 N=3192 N=3148 N=1691 Placebo N=3301 N=3258 N=3221 N=3174 N=3108 N=1659 Coronary Revascularizations 0.05 0.04 33% Risk Reduction (p = 0.001) Placebo 0.03 Cumulative Incidence 0.02 Lovastatin 0.01 0.00 0 1 2 3 4 5 5+ Years Years of Follow-up JAMA 1998;279:1615-1622
Mortality Placebo Lovastatin Event n=3301 n=3304 P-value Total Mortality 77 80 N.S. Cardiovascular 25 17 too few* Non-cardiovascular 52 63 N.S. *Too few for survival analyses JAMA 1998;279:1615-1622
Tertiary Analysis Fatal and Non-Fatal Cancer* 0.08 *Excludes non-melanoma skin cancer 0.07 P = NS Placebo 0.06 0.05 Lovastatin Cumulative Incidence 0.04 0.03 0.02 0.01 0.00 0 1 2 3 4 5 5+ years Years of Follow-up # At Risk Lovastatin N=3304 N=3249 N=3188 N=3117 N=3059 N=1626 Poster Presentation 1998 ACC Meeting, Atlanta GA Placebo N=3301 N=3234 N=3171 N=3105 N=3043 N=1603
Cancer Placebo Lovastatin n=3301 n=3304 P-value All Fatal and Non-Fatal 259 252 .75 Most Frequently Reported Prostate 108 109 > 0.99 Melanoma 27 14 0.04 Colon 20 25 .55 Lung 17 22 .52 Lymphoma 11 12 > 0.99 Bladder 11 12 > 0.99 Breast 9 13 .52 JAMA 1998;279:1615-1622
Safety ~ Laboratory *Consecutive elevations #Treatment group differences were not significant JAMA 1998;279:1615-1622
Summary of Results • Men and women who are free of clinical evidence of atherosclerotic CVD, with average TC and LDL-C but below average HDL-C can obtain significant benefit from LDL-C reduction with lovastatin 20-40 mg/day. • Lovastatin 20-40 mg/day, (mean dose 30 mg/day) significantly reduced the risk of: • The first acute major coronary event - by 37 % (p<0.001) • MI - by 40% (p=0.002) • Unstable angina - by 32% (p=0.02) • Coronary revascularization - by 33 % (p=0.001) • Was generally well-tolerated (13.6% discontinuation rate compared with 13.8% for placebo) JAMA 1998;279:1615-1622
Summary of Results • Clinical benefit • Appeared within the first year of treatment and continued • Was apparent for all LDL-C tertiles • Range 90-235 mg/dl • Was consistent for subgroups • Women • Risk Factors - Age, DM, HTN, Smokers JAMA 1998;279:1615-1622
Conclusions • In conjunction with a prudent diet, regular exercise and risk factor modification Lovastatin 20-40 mg/day could be used to lower the risk of the first acute major coronary event • for primary prevention candidates - • men > 45 years, women > 55 years • HDL < 50 mg/dl • LDL > 130 mg/dl JAMA 1998;279:1615-1622
Conclusions • Lovastatin 20-40 mg/day reduces the risk for the first acute major coronary event in men and women with average TC and LDL-C and below-average HDL-C • These findings support the inclusion of HDL-C in risk-factor assessment and confirm the benefit of LDL-C reduction to a target goal JAMA 1998;279:1615-1622
Conclusions • Treatment was beneficial for women, and persons with any active risk factor and appeared to neutralize the risk conferred by HTN, smoking and low HDL JAMA 1998;279:1615-1622
AFCAPS/TexCAPSImplications • “Using NHANES III survey data, approximately 8 million Americans without documented cardiovascular disease meet the age and lipid criteria of AFCAPS/TexCAPS.” • “Assuming that only 17% of the reference population would qualify for drug treatment by current NCEP guidelines, we estimate that 6 million Americans currently not recommended for drug treatment may benefit from LDL-C reduction with lovastatin.” JAMA 1998;279:1615-1622
Cost Analysis (AFCAPS/TexCAPS) • Cost of hospitalizations, procedures, etc.* • Placebo group = $2,100 • Lovastatin group = $1,513 • Savings = $587 per patient during study • Cost of lovastatin therapy (retail price x days on drug) • $4,700 • Cost per day of lovastatin (offset by savings) • $2.44 *Does not include loss of income, non-medical expenses, etc. Gotto, ACC, Atlanta, GA 1998